PATIENT RESOURCES
CONDITIONS & INJURIES
Common Conditions we treat:
DESCRIPTION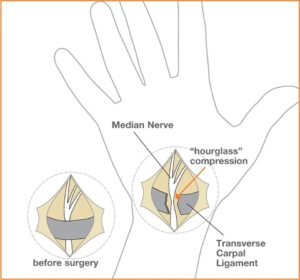
Carpal tunnel syndrome is essentially a pinched nerve in the wrist. There is a space in the wrist called the carpal tunnel where the median nerve and nine tendons pass from the forearm into the hand (Figure 1). Carpal tunnel syndrome happens when swelling in this tunnel puts pressure on the nerve.
CAUSES
Pressure on the nerve can happen several ways, including:
- Swelling of the lining of the flexor tendons, called tenosynovitis
- Joint dislocations
- Fractures
- Arthritis
- Fluid build-up during pregnancy
The scenarios listed above can narrow the carpal tunnel or cause swelling in the tunnel. Thyroid conditions, rheumatoid arthritis and diabetes can also be associated with carpal tunnel syndrome. Ultimately, there can be many causes of this condition.
SIGNS & SYMPTOMS
Symptoms of this condition can include:
- Pain
- Numbness
- Tingling
- Weak grip
- Occasional clumsiness
- Tendency to drop things
The numbness or tingling most often takes place in the thumb, index, middle and ring fingers. The symptoms usually are felt during the night but may also be noticed during daily activities such as driving or reading a newspaper. In bad cases, sensation and strength may be permanently lost.
How your doctor will diagnose Carpal Tunnel
A detailed history including medical conditions, how the hands have been used, and any prior injuries is important in diagnosing carpal tunnel syndrome. An x-ray may be taken to check for arthritis or a fracture. In some cases, laboratory tests may be done. Electrodiagnostic studies are also a possibility to confirm the diagnosis and check for other possible nerve problems.
TREATMENT
Symptoms may often be relieved without surgery. Some treatment options are:
- Changing patterns of hand use (helps reduce pressure on the nerve)
- Keeping the wrist splinted in a straight position (helps reduce pressure on the nerve)
- Wearing wrist splints at night (helps relieve symptoms that may prevent sleep)
- Steroid injections into the carpal tunnel (helps reduce swelling around the nerve)
When symptoms are severe or do not improve, surgery may be needed to make more room for the nerve. Pressure on the nerve is decreased by cutting the ligament that forms the top of the tunnel on the palm side of the hand (Figure 2). Following surgery, soreness around the cut area may last for several weeks or months. The numbness and tingling may disappear quickly or slowly. Recovery may take several months. Carpal tunnel symptoms may not completely go away after surgery, especially in severe cases.
© 2012 American Society for Surgery of the Hand

DESCRIPTION
These cysts may change in size or even disappear completely, and they may or may not be painful. These cysts are not cancerous and will not spread to other areas.
TREATMENT
Treatment can often be non-surgical. In many cases, these cysts can simply be observed, especially if they are painless, as they frequently disappear spontaneously. If the cyst becomes painful, limits activity, or is otherwise unacceptable, several treatment options are available. The use of splints and anti-inflammatory medication can be prescribed in order to decrease pain associated with activities. An aspiration can be performed to remove the fluid from the cyst and decompress it. This requires placing a needle into the cyst, which can be performed in most office settings. Aspiration is a very simple procedure, but recurrence of the cyst is common. If non-surgical options fail to provide relief or if the cyst recurs, surgical alternatives are available. Surgery involves removing the cyst along with a portion of the joint capsule or tendon sheath (see Figure 3). In the case of wrist ganglion cysts, both traditional open and arthroscopic techniques usually yield good results. Surgical treatment is generally successful although cysts may recur. Your surgeon will discuss the best treatment options for you.
Figure 1: Ganglion top side (dorsum) wrist
Figure 2: Ganglion end joint of finger (mucous cyst)

Figure 3: Cross-section of wrist showing stalk (or root) of ganglion.
© 2012 American Society for Surgery of the Hand

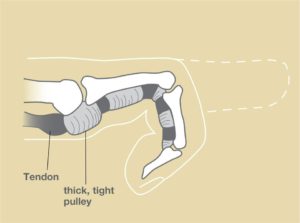
Stenosing tenosynovitis is a condition commonly known as “trigger finger.” It is sometimes also called “trigger thumb.” The tendons that bend the fingers glide easily with the help of pulleys. These pulleys hold the tendons close to the bone. This is similar to how a line is held on a fishing rod (Figure 1). Trigger finger occurs when the pulley becomes too thick, so the tendon cannot glide easily through it (Figure 2).
- Pain
- Popping
- Catching feeling
- Limited finger movement
Common treatments include, but are not limited to:
- Night splints
- Anti-inflammatory medication
- Changing your activity
- Steroid injection
If non-surgical treatments do not relieve the symptoms, surgery may be recommended. The goal of surgery is to open the pulley at the base of the finger so that the tendon can glide more freely. The clicking or popping goes away first. Finger motion can return quickly, or there can be some stiffness after surgery. Occasionally, hand therapy is required after surgery to regain better use.
© 2015 American Society for Surgery of the Hand 
Patients with thumb arthritis report pain and weakness with pinching and grasping. For instance, opening jars, turning doorknobs or keys, and writing are often painful.
The diagnosis is made by talking with you and examining you. The appearance of the thumb can change with the development of bone spurs and stretching of soft tissues (ligaments) . A grinding sensation may also be present at the joint. X-rays are not necessary to make the diagnosis, but they can help you understand the disease and they can help when surgery is being considered.
TREATMENT
As with other aspects of aging, we adapt to thumb arthritis and treatment is often unnecessary. Options for treatment include non-surgical methods and surgery. Treatments without surgery range from ice/heat, pain medicines, splinting, and injections.
Surgery consists of removing the joint either by removing a bone or connecting the bones together. There are options for moving one of your tendons to secure or cushion the bone, and each hand surgeon has a different opinion on whether this is helpful. After surgery, a splint or cast is worn for several weeks.
(c) 2013 American Society for Surgery of the Hand
Developed by the ASSH Public Education Committee
All Conditions:

The major concern of all bite wounds is subsequent infection. In the United States, about 1% of dog bites and about 5-10% of cat bites require hospitalization. With swift and proper care, the prognosis is usually very good for recovery from these injuries.
Rabies is an extremely rare but fatal infection that may result from an animal bite. In the United States, unlike the rest of the world, wild animals such as bats, skunks, raccoons, and foxes spread more than 90% of rabies infections. All bites should be reported to your local health department. They may ask your assistance in locating the animal so that it can be confined and observed for symptoms of rabies.
Human Bites (Clenched fist injury)
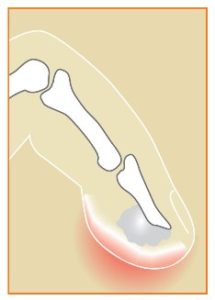
Human bite wounds contain very high concentrations of bacteria so the risk of infection is high. These infections can progress rapidly and result in substantial complications, so early treatment is necessary (see Figure 2). Often, human bites occur when a person’s fist is driven into another person’s mouth, such as during a fistfight. After the skin is broken, bacteria are seeded into the soft tissue and often into the “knuckle” joint, which if left untreated often results in deep infection of the joint that may ultimately destroy the joint. The extensor tendon is often cut by the victim’s tooth. The tooth may even break and be left in the wound. Early diagnosis, intravenous antibiotics, and surgery to drain the infection and wash out the joint can effectively treat these injuries.
Bites to the hand require meticulous cleansing. Your doctor or other medical personnel will wash the wound and might trim away any devitalized (dead) tissue, damaged skin, blood clots, or other particles that could be a source of infection. It is important to look for signs of lymphangitis, indicated by the presence of red streaks up the forearm. When the wound is infected, a culture is obtained to identify the type of bacteria that is causing the infection and thus help determine the antibiotic that is most effective for treatment.
The use of antibiotics for animal bites depends on the particular circumstances of the injury, patient health, and sensitivity to various medications, and the appearance of the wound. Some bites require the use of intravenous (IV) antibiotics, while others may be treated with oral medications. The presence of an underlying fracture usually dictates inpatient antibiotic treatment. If you are diagnosed as having an infection of a flexor tendon sheath or joint, you will need to have hand surgery, which would need to be performed as soon as possible.
Follow-up care is crucial in the case of animal or human bite wounds, to ensure that infection is diminishing or has not developed, and to restore the hand as best as possible to its former condition. These injuries should be taken seriously to prevent poor function of your hand.
© 2006 American Society for Surgery of the Hand

- Wrist, specifically the distal radius
- Forearm bones (radius and ulna) (Figure 1A)
- Elbow
- Humerus
- Shoulder
- Bruised
- Painful
- Swollen
- Difficult to move
- Numb or tingly
Any deep cuts that might be associated with a broken bone should also be checked immediately since there is a risk of infection with broken bones that come through the skin.
Diagnosis
The doctor will check to make sure the nerves and blood vessels are okay. An x-ray is usually taken to diagnose a broken bone. Sometimes more studies, such as a CT scan or MRI, will be recommended.
If the fracture is out of place, a doctor may try to straighten it (“reduce” the fracture). This is often done in the emergency department or within a few days after the break happens. In most cases, follow-up with a hand surgeon will be recommended.
Many times, especially in children, broken arms heal well in a cast (Figure 2). The cast is usually on for 4-6 weeks, after which activities may be restricted for 2-3 months. With certain types of breaks, or if a cast won’t be effective, the doctor may recommend surgery to straighten the bones and put in pins, screws, plates or other devices to hold the bones in place while they heal (Figure 1B and 1C).
Hand therapy is often recommended to help regain the range of motion and strength following a broken arm. In some simple fractures, it is expected that nearly all of the strength and motion can be recovered. In more complicated breaks, it is not uncommon to lose some motion as compared to the other arm. In severe cases, arthritis with pain and stiffness may result, even despite the best attempts to straighten the bones. In some cases, more surgery is eventually necessary.
Hand surgeons are specially trained to diagnose and treat fractures in the upper extremity. Visit a hand surgeon if you have injured your arm.
Figure 1A: An x-ray of an ulna fracture
Figure 1B and 1C: Pins and screws holding the ulna in place
Figure 2: A broken radius and ulna in a child and the healed bones after being treated with a cast
© 2015 American Society for Surgery of the Hand
DESCRIPTION
Carpal tunnel syndrome is essentially a pinched nerve in the wrist. There is a space in the wrist called the carpal tunnel where the median nerve and nine tendons pass from the forearm into the hand (Figure 1). Carpal tunnel syndrome happens when swelling in this tunnel puts pressure on the nerve.
CAUSES
Pressure on the nerve can happen several ways, including:
- Swelling of the lining of the flexor tendons, called tenosynovitis
- Joint dislocations
- Fractures
- Arthritis
- Fluid build-up during pregnancy
The scenarios listed above can narrow the carpal tunnel or cause swelling in the tunnel. Thyroid conditions, rheumatoid arthritis and diabetes can also be associated with carpal tunnel syndrome. Ultimately, there can be many causes of this condition.
SIGNS & SYMPTOMS
Symptoms of this condition can include:
- Pain
- Numbness
- Tingling
- Weak grip
- Occasional clumsiness
- Tendency to drop things
The numbness or tingling most often takes place in the thumb, index, middle and ring fingers. The symptoms usually are felt during the night but may also be noticed during daily activities such as driving or reading a newspaper. In bad cases, sensation and strength may be permanently lost.
How your doctor will diagnose Carpal Tunnel
A detailed history including medical conditions, how the hands have been used, and any prior injuries is important in diagnosing carpal tunnel syndrome. An x-ray may be taken to check for arthritis or a fracture. In some cases, laboratory tests may be done. Electrodiagnostic studies are also a possibility to confirm the diagnosis and check for other possible nerve problems.
TREATMENT
Symptoms may often be relieved without surgery. Some treatment options are:
- Changing patterns of hand use (helps reduce pressure on the nerve)
- Keeping the wrist splinted in a straight position (helps reduce pressure on the nerve)
- Wearing wrist splints at night (helps relieve symptoms that may prevent sleep)
- Steroid injections into the carpal tunnel (helps reduce swelling around the nerve)
When symptoms are severe or do not improve, surgery may be needed to make more room for the nerve. Pressure on the nerve is decreased by cutting the ligament that forms the top of the tunnel on the palm side of the hand (Figure 2). Following surgery, soreness around the cut area may last for several weeks or months. The numbness and tingling may disappear quickly or slowly. Recovery may take several months. Carpal tunnel symptoms may not completely go away after surgery, especially in severe cases.
© 2012 American Society for Surgery of the Hand
The causes of CRPS are not known. CRPS can begin after a minor injury, such as a sprain or small cut, or after major trauma or surgery. Injury to a nerve may also cause the condition. It is most common among individuals between 25 and 55 years of age, though anyone of any age can be affected. CRPS is three times more likely to occur in women than men. An estimated 60,000 Americans are affected by CRPS.
- “Burning” pain
- Sensitive skin
- Changes in skin temperature (warmer or cooler compared to other parts of the body)
- Changes in skin color (often blotchy, purple, pale or red)
- Changes in skin texture (shiny and thin, and sometimes excessively sweaty)
- Changes in nail and hair growth patterns
- Swelling and stiffness in affected joints
- Decreased ability to move the affected body part
The pain may spread to include the entire arm or leg, even though the initial injury might have been only to a finger or toe. Pain can sometimes even travel to the other hand, arm or leg. It may get worse with emotional stress.
There is no single test to confirm that you have CRPS. The diagnosis is primarily through observation of signs and symptoms. Patients must be examined by a qualified physician who does a thorough history and physical examination. X-rays, MRI, EMG/NCV, bone scans, thermography, or pain imaging (where available) may be helpful. You may need to visit another specialist, and a pain clinic is often recommended.
The earlier the diagnosis of CRPS is made and treatment started, the better the chance for recovery. Treatment is varied and depends on both the symptoms and amount of time that has passed. Exercise, treating possible sleep disorders, and treating possible psychological problems can be helpful for treatment. Since there is no simple cure for CRPS, treatment is intended to relieve painful symptoms so that patients can resume their normal lives and use their hands or arms normally.
Some CRPS treatments include:
- Occupational/Physical Therapy: An increasing exercise program may help preserve or restore the function of your hand. Overall, exercise is very important to improve symptoms.
- Psychotherapy: CRPS can have psychological effects on patients and their families. Many with CRPS have depression, anxiety or post-traumatic stress disorder. A psychologist or psychiatrist may be able to help with this issue.
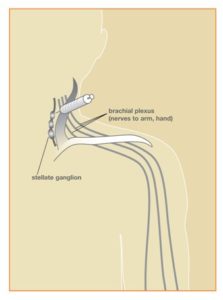
- Nerve Blocks: Many patients experience significant relief from this treatment. A nerve block is when an anesthetic is injected to numb the nerves. This can relieve pain, improve mood, and improve level of activity. An example of a stellate ganglion block is shown in Figure 1.
- Medications: Many different drugs are used to treat CRPS and other conditions such as sleep disorders, depression and anxiety. Medications may include anti-seizure drugs, antidepressants, corticosteroids, muscle relaxants, and sleeping medications.
- Surgery: If the CRPS is from a compressed nerve, such as with carpal tunnel syndrome, then surgery to release pressure on the nerve may be needed (e.g. carpal tunnel release).
Discuss your treatment options with your physician. Each patient with CRPS responds differently to treatment. Most physicians believe that early treatment is helpful to limit the disability from CRPS. More research is needed to understand the causes, the development of the disease, and how treatment can alter its course.
© 2012 American Society for Surgery of the Hand
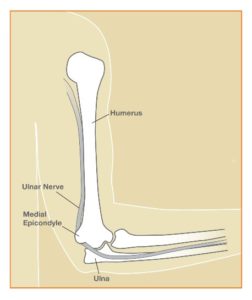
- Pressure: The nerve has little padding over it. Direct pressure (like leaning the arm on an arm rest) can press the nerve, causing the arm and hand — especially the ring and small fingers — to “fall asleep.”
- Stretching: Keeping the elbow bent for a long time can stretch the nerve behind the elbow. This can happen during sleep.
- Anatomy: Sometimes, the ulnar nerve does not stay in its place and snaps back and forth over a bony bump as the elbow is moved. Repeated snapping can irritate the nerve. Sometimes, the soft tissues over the nerve become thicker or there is an “extra” muscle over the nerve that can keep it from working correctly.
Diagnosis
Your doctor can learn much by asking you about your symptoms and examining you. S/he might test you for other medical problems like diabetes or thyroid disease. Sometimes, nerve testing (EMG/NCS) may be needed to see how much the nerve and muscle are being affected. This test also checks for other problems such as a pinched nerve in the neck, which can cause similar symptoms.
Sometimes, surgery may be needed to relieve the pressure on the nerve. This can involve releasing the nerve, moving the nerve to the front of the elbow, and/or removing a part of the bone. Your surgeon will talk to you about options.
Therapy is sometimes needed after surgery, and the time it takes to recover can vary. Numbness and tingling may improve quickly or slowly. It may take many months for recovery after surgery. Cubital tunnel symptoms may not totally go away after surgery, especially if symptoms are severe.
© 2015 American Society for Surgery of the Hand
A splint that stops you from moving your thumb and wrist.
Tylenol or aspirin type medications (e.g., ibuprofen).
Treatments that attempt to change the course of the disease include:
A cortisone-type of steroid injection into the tendon compartment. It has not been clearly established that these injections change the course of the disease and response to the injection varies.
Surgery to open the tunnel and make more room for the tendons.
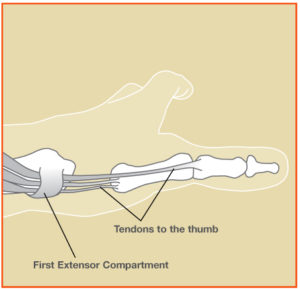
Figure 1A: The first dorsal compartment. There are six compartments on the dorsal, or back, side of the wrist. The first and third compartments house tendons that control the thumb.
Figure 1B: A drawing of the first dorsal compartment.
Figure 2A and B: Pain with this motion (a hammering motion with the thumb in the fist) is characteristic of de Quervain syndrome.
© 2012 American Society for Surgery of the Hand. Developed by the ASSH Public Education Committee
The cause of Dupuytren’s contracture is unknown. The problem is more common in men, people over age 40 and people of northern European descent. There is no proven evidence that hand injuries or specific jobs lead to a higher risk of developing Dupuytren’s contracture .
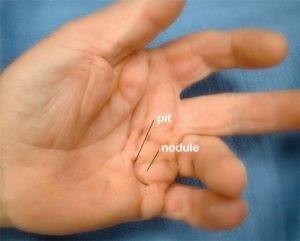
The lumps can be uncomfortable in some people, but Dupuytren’s contracture is not typically painful. The disease may first be noticed because of difficulty placing the hand flat on a surface (Figure 3). As the fingers are drawn into the palm, it may be more difficult to wash hands, wear gloves, shake hands, and get hands into pockets. It is difficult to predict how the disease will progress. Some people have only small lumps or cords while others will develop severely bent fingers. The disease tends to be more severe if it occurs at an earlier age.
Your hand surgeon will discuss the most appropriate method based upon the stage and pattern of the disease and the joints involved. The goal of treatment is to improve finger motion and function; however, complete correction of the finger(s) may not always happen. Even with treatment, the disease may come back. Before treatment, the surgeon will discuss realistic goals and possible risks.
Splinting and hand therapy are often needed after treatment in order to maintain the improved finger function.
Figure 1: Advanced case of Dupuytren with pits, nodules and cords leading to bending of the finger into the palm
© 2015 American Society for Surgery of the Hand
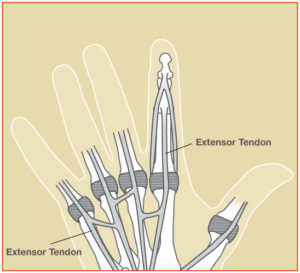
Common Extensor Tendon Injuries
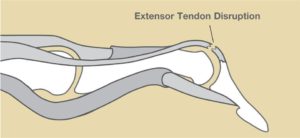
- Mallet Fingerrefers to a drooping end-joint of a finger. This happens when an extensor tendon has been cut or torn from the bone (Figure 2). It is common when a ball or other object strikes the tip of the finger or thumb and forcibly bends it.
- Boutonnière Deformity describes the bent-down (flexed) position of the middle joint of the finger. Boutonniere can happen from a cut or tear of the extensor tendon (Figure 3).
- Cuts on the back of the hand can injure the extensor tendons. This can make it difficult to straighten your fingers.
Other treatment may include stitches (for cuts in the tendon). Also, a pin may need to be placed through the bone across the joint as an internal splint. Surgery to free scar tissue is sometimes helpful in cases of severe motion loss.
After treatment, therapy may be necessary to improve motion. Consult your hand specialist for the best form of treatment.
© 2014 American Society for Surgery of the Hand
Fingertip injuries are one of the more common injuries in the hand. The fingertips are exposed in many of our activities. They can be crushed, such as by a closing door, a hammer, or a heavy object dropped onto the finger. They can be cut with a knife or power tool, such as a saw, sander, lawnmower, or snowblower. There are many ways to obtain a fingertip injury.
When patients lose more than skin and have exposed bone, the injury may need to be covered with a flap of skin that has some soft tissue with it for padding. Small wounds on the tip of the finger may be covered with a flap from the injured finger. Larger wounds, such as those that result in substantial loss of the pulp, require a flap that is elevated from an adjacent finger (see Figure 2) or other source. The flap remains attached to its original site so that it has blood supply while it is stitched to the finger wound. A skin graft is used to cover the donor site defect. After a few weeks the flap has sufficient blood supply coming from the injured finger as it heals into its new location, and can be divided from its origin and fully set into the wound.
Fractures of the bone in the tip of the finger are common. Very small fractures of the end or tuft of the bone usually do not affect the strength of the bone. Repair of the soft tissue, such as the nail bed, usually re-aligns and stabilizes these bone fragments. Fractures closer to the joint may require a splint or even a temporary metal pin(s) to hold the bone fragments in proper position. If the damage is too severe, amputation of the fingertip may be necessary.
Fingertip sensitivity is common and may last for many months. Sometimes the feeling in the fingertip is limited. The contour may have some distortion, and the quality and texture of the skin may be different than the very specialized skin that normally covers the fingertip. There also may be some deformity at the donor site of a graft or flap. Stiffness can be a concern, especially if a flap is needed.
If there is a nailbed injury that is sharp and can be repaired, a normal nail is likely. If there is more severe crushing of the nail bed, then there is a greater likelihood of nail bed scarring and subsequent deformity of the nail (see brochure or web page on Nailbed Injuries).
(c) 2007 American Society for Surgery of the Hand. Developed by the ASSH Public Education Committee

In most cases, exercise is done by having you move your fingers with your other hand, but you are not allowed to try to bend your finger on your own for about a month. You must wear a splint for at least a month after surgery. These exercises can be tricky and a hand therapist can help you. These exercises can vary among surgeons; your surgeon will direct your care.
Prognosis
There is scarring as the tendon heals, and most people do not regain normal motion. In some cases, if motion is less than expected after months of exercises, then your surgeon might offer you surgery to release scar tissue around the tendon.
© 2013 American Society for Surgery of the Hand.
Developed by the ASSH Public Education Committee
These cysts may change in size or even disappear completely, and they may or may not be painful. These cysts are not cancerous and will not spread to other areas.
Figure : Cross-section of wrist showing stalk (or root) of ganglion.
© 2012 American Society for Surgery of the Hand
Proper warm up and stretching is important to decrease the chance of injury while golfing. Gradually increasing the length and intensity of play as the season progresses can help avoid overuse injuries. Conditioning and core muscle strengthening can improve swing mechanics. Instruction with a teaching professional will refine your technique and increase your enjoyment of the game injury free.
Types of Golf Injuries
Golf injuries can include tendonitis, sprains or fractures (broken bones).
- Sprains or ligament injuries to the wrist most often involve pain and popping in the wrist.
- Wrist tendonitis typically occurs in the leading hand (left hand for a right handed player).
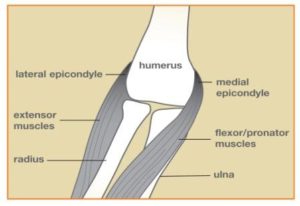
- Medial Epicondylitis, also known as “golfer’s elbow,” is a painful tendonitis on the inner aspect of the elbow, where the muscles that bend the wrist and fingers attach (Figure 1). Tendonitis on the outer aspect of the elbow (Lateral Epicondylitis) is more common.
- Hamate bone fractures occur when the club strikes the ground, forcing the handle against the bony hook (Figures 2, 3 and 4). The hook part of the bone can break, causing pain in the heel of the hand.
- Damaged blood vessels can happen from the club handle repeatedly striking the palm. Hypothenar Hammer Syndrome describes an injury to one of the main arteries to the hand, where repeated blows weaken the vessel wall causing it to enlarge and sometimes to clot. This can cause local pain in the palm or disrupt blood flow going to the fingertips, producing pain, numbness and color changes in the fingertips.
These injuries may arise by the repeated stress of practicing the golf swing or by similar gripping activities such as hammering and heavy lifting.
When symptoms persist, a cortisone injection may be used to reduce the painful area. Your doctor can assist you with this decision. For some patients, a surgical procedure (often with wrist arthroscopy) may be recommended. Casting may also be necessary for fractures.
© 2014 American Society for Surgery of the Hand

Causes of Gout
Crystals form when people make too much, or do not get rid of, uric acid. Genetics are the main factor in determining uric acid levels. However, some medicines can cause changes in uric acid levels, including medicine for high blood pressure, diuretics (water pills), some blood thinners, and a medicine called cyclosporine, which is used for patients who have had a transplanted organ. Eating meat, seafood, and alcohol can also raise uric acid levels. In addition, obesity, insulin resistance, high cholesterol, heart disease, hypothyroidism and kidney disease can be associated with with this type of arthritis. Episodes of this condition have been noted after injury or surgery, sometimes involving infection or the use of contrast for x-rays. Physical fitness seems to help with prevention.Causes of Pseudogout
With this type of arthritis, sometimes known as calcium pyrophosphate deposition (CPPD), many people will form the crystals throughout their life, but most will not have pain, swelling or redness. It is not clear why this only becomes a problem for certain people. Symptoms are more common with age, in people who have a history of injury to a joint, and in those with a family history of these problems. Unlike gout, pseudogout is not connected with alcohol or diet and is not caused by medicine. It can occur with certain problems like pneumonia, heart attacks, and strokes, and it may occur after an unrelated surgery. It has been found in people with thyroid problems, in people who have problems with parathyroid glands, and in those with high calcium and iron.Gout crystals can form white bumps called “tophi” that are often visible under the skin (Figure 2). The crystals in pseudogout are usually only visible on an x-ray (Figure 3).
The diagnosis for either disease is made based on a physical examination by your doctor, x-rays, and lab tests. You will be asked about your symptoms and how the disease has changed your activities. Because medications and other diseases can cause this condition, you will be asked to provide a medical history and a medication list.
X-rays are also helpful. Calcium in pseudogout can be seen on an x-ray. Uric acid does not show up on x-rays, but some bone changes can be visible with gout (Figure 4). If needed, fluid from the joint can be removed with a needle to confirm the diagnosis. Blood tests may be ordered to check for infection as well as uric acid levels.
Episodes of can come and go. When the episodes are infrequent, an NSAID or colchicine can be used as needed. For more frequent episodes, a specific medicine can be managed by your primary care doctor or a rheumatologist.
These conditions are usually treated without surgery. There are medicines, splints, and compressions to help swelling and lessen pain. If the disease has worn out the joints or if tendons have been hurt, surgery may be needed.
If gout is not treated, the inflammation can cause damage to joints and tendons. Crystal deposits on tendons can cause the skin to wear down, which can lead to infection. In addition, tendons can tear, which can lead to loss of function.
Pseudogout crystals are less likely to be deposited under the skin, so some of the problems seen with gout are less likely. The crystals in ligaments and cartilage may lead to joint injury. Loss of motion is common.
© 2013 American Society for Surgery of the Hand
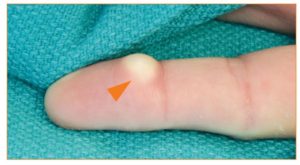
Common Types of Wrist Hand Tumors
- Ganglion Cysts (Figure 1): This is the most common tumor in the hand and wrist. Ganglion cysts are seen frequently in the wrist but can occur at the base of the fingers or around the finger joints. The cyst is typically filled with fluid, and it will feel very firm. There are several treatment options for a ganglion cyst, including observation (doing nothing), aspiration (puncturing with a needle) or surgically removing it.
- Giant cell tumor of the tendon sheath (Figure 2): This is the second most common hand tumor. Unlike the fluid-filled ganglion cyst, these tumors are solid. They are benign (not cancer) and slow-growing.
- Epidermal inclusion cyst (Figure 3): This tumor is benign and forms just underneath the skin where there may have been a cut or puncture. The cyst is filled with keratin, a soft, waxy material.
There are other less common types of tumors seen in the hand, including lipomas (fatty tumors), neuromas (nerve tumors), nerve sheath tumors, fibromas and glomus tumors, among others. Almost all are benign.
Other Causes of Lumps, Bumps and Masses
Foreign bodies, such as a splinter, can cause reactions that form bumps in the hand. Dupuytren’s Contracture may cause firm bumps in the hand, which are often confused with tumors (Figure 4). Finally, blood vessel growths can also be confused with other tumors.
How Your Doctor Will Diagnose
A physical exam and review of your medical history by a hand surgeon can help to determine the type of hand or wrist tumor you may have. X-rays might be taken to evaluate the bones, joints and possibly the soft tissue. Further studies such as ultrasound, CT, MRI or bone scans may be done to help narrow down the diagnosis. Needle biopsy or incisional biopsy (cutting out a small sample of the tumor) may be considered if the surgeon wants to confirm the diagnosis before recommending treatment.
Typically, the most successful treatment is removing the tumor with surgery. This allows a pathologist to analyze it and to determine the type of tumor. Often, surgery is done on an outpatient basis.
Some patients may choose to do nothing and simply live with the tumor once they learn that it is non-cancerous. However, if the tumor changes (e.g. skin discoloration, pain, increased size) or if it causes other problems such as numbness or pain from pressure on a nearby nerve, then re-evaluation by a hand surgeon is recommended. You and your hand surgeon can choose the best treatment plan.
© 2015 American Society for Surgery of the Hand
A splint or cast may be used to treat a fracture that is not displaced, or to protect a fracture that has been set. Some displaced fractures may need to be set and then held in place with wires or pins without making an incision. This is called closed reduction and internal fixation.
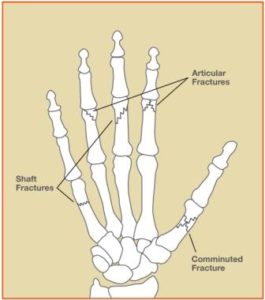
Other fractures may need surgery to set the bone (open reduction). Once the bone fragments are set, they are held together with pins, plates, or screws (see Figure 2). Fractures that disrupt the joint surface (articular fractures) usually need to be set more precisely to restore the joint surface as smooth as possible. On occasion, bone may be missing or be so severely crushed that it cannot be repaired. In such cases, a bone graft may be necessary. In this procedure, bone is taken from another part of the body to help provide more stability. Sometimes bone graft substitutes may be used instead of taking bone from another part of the body.
Fractures that have been set may be held in place by an “external fixator,” a set of metal bars outside the body attached to pins which are placed in the bone above and below the fracture site, in effect keeping it in traction until the bone heals.
Once the fracture has enough stability, motion exercises may be started to try to avoid stiffness. Your hand surgeon can determine when the fracture is sufficiently stable.
What types of results can I expect from surgery for hand fractures?
Perfect alignment of the bone on x-ray is not always necessary to get good function. A bony lump may appear at the fracture site as the bone heals and is known as a “fracture callus.” This functions as a “spot weld.” This is a normal healing process and the lump usually gets smaller over time. Problems with fracture healing include stiffness, shift in position, infection, slow healing, or complete failure to heal. Smoking has been shown to slow fracture healing. Fractures in children occasionally affect future growth of that bone (see the brochure/web page on Fractures in Children). You can lessen the chances of complication by carefully following your hand surgeon’s advice during the healing process and before returning to work or sports activities. A hand therapy program with splints and exercises may be recommended by your physician to speed and improve the recovery process.
© 2006 American Society for Surgery of the Hand. Developed by the ASSH Public Education Committee
Atypical Mycobacterial Infections
Rarely, a hand infection can be caused by an “atypical mycobacterium.” One of the more common types, Mycobacterium marinum infection, can develop after puncture wounds from fish spines or contamination of a simple wound or abrasion from stagnant water (in nature or from aquariums). These atypical infections develop gradually and may be associated with swelling and stiffness without much pain or redness. Surgical removal of infected tissue may be necessary and is helpful to determine which medicine will help treat the infection; often the medical treatment lasts several months. Patients whose immune systems are not working well (for example, those undergoing chemotherapy or who have HIV) are more susceptible to atypical mycobacterial infections.Bite Wound Infections
Cellulitis
Deep Space Infections
Felon
Herpetic Whitlow
MRSA
Necrotizing Fasciitis, or “Flesh-Eating Bacteria”
Paronychia
Septic Arthritis/Osteomyelitis
Tendon Sheath Infection (“Infectious Tenosynovitis”)
© 2013 American Society for Surgery of the Hand
DESCRIPTION
Hand Therapy is a type of rehabilitation performed by an occupational or physical therapist with patients that suffer from conditions affecting the hands and upper extremities. Therapy enables patients to hasten their return to a productive lifestyle.
Patients who are candidates for hand therapy may have been affected by an accident or trauma leaving them with wounds, scars, burns, injured tendons or nerves, fractures, or even amputations of the fingers, hands or arms. Others include patients who suffer from conditions such as carpal tunnel syndrome and tennis elbow, as well as from chronic problems such as arthritis or a neurologic condition (i.e. stroke).
What Does Hand Therapy Provide?
- Treatments without an operation
- Help with recent or long-lasting pain
- Help to reduce sensitivity from nerve problems
- Learning to feel again after a nerve injury
- Learning home exercise programs to help with movement and strength
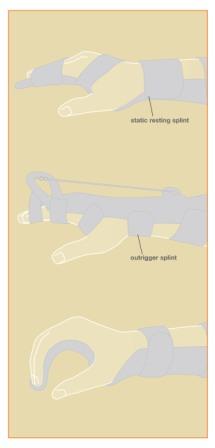
- How to make splints to help prevent or improve stiffness (Figure 1)
- Learning to complete everyday activities with special tools
- Help getting back to work
If surgery is needed, hand therapists can also help with a patient’s recovery. This may include assistance with helping wounds heal, preventing infection, scar management and reducing swelling.
Getting Back to Work
Hand therapists are able to talk with employers about preventing problems for workers with hand or arm symptoms. They may recommend changes at your place of work or different ways of doing your job to help ensure a healthy style of work.
Find a Hand Therapist
Search for a hand therapist in your area by going to www.asht.org, the official website of the American Society of Hand Therapists.
© 2014 American Society for Surgery of the Hand. Content provided by the American Society of Hand Therapists.

Other injuries that may occur from more violent forces include torn tendons, fractures (broken bones) and dislocations (Figure 1).
Jammed fingers may be treated without or with surgery, depending on how severe the injury is. Some injuries can be treated with a splint and/or buddy strapping to the neighboring normal finger (Figure 2). These treatments are often performed along with the care of a hand therapist. Some severe injuries require surgery. In any case, even with simple sprains, the finger may be swollen for up to a full year. You and your hand specialist will determine the best approach for your individual situation. Successful outcomes depend on the combined efforts of the specialist, therapist and you.
© 2015 American Society for Surgery of the Hand

. Its origin may involve multiple factors, such as the blood supply (arteries), the blood drainage (veins), and skeletal variations. Skeletal variations associated with this disease include a shorter length of the ulna, one of the forearm bones, and also the shape of the lunate bone itself (see Figure 2). Trauma, either single or repeated episodes, may possibly be a factor in some cases. This disease can be found more commonly in people who have medical conditions that affect blood supply, and it is also associated with diseases like lupus, sickle cell anemia, and cerebral palsy.
Most patients with this disease initially present with wrist pain. There is usually tenderness directly over the lunate bone, decreased motion or stiffness of the wrist, and there can be swelling. The diagnosis of this disease can often be made by history, physical examination, and plain x-rays. In early stages the x-rays may be normal and special studies are needed to confirm the diagnosis. Probably the most reliable special study to assess the blood supply of the lunate is Magnetic Resonance Imaging, or MRI (Figure 3). CT scanning, specialized CT scanning, and bone scan may also be used.
Patients often have the condition for months or even years before they seek treatment, and especially in its earlier stage it can be difficult to diagnose.
The progression of this disease varies but is usually slow over many years. There are 4 stages used to classify avascular necrosis of the lunate. In stage 1, x-rays appear normal, but the lunate has lost its blood supply and is painful and may fracture. In stage 2 the bone hardens due to lack of blood supply and appears abnormally dense on X-ray. In stage 3 the bone collapses and fragments. In the final stage, stage 4, the lunate is collapsed and the bones around the lunate have developed degenerative changes and become arthritic. In the early stages there may be only pain and swelling, but as the disease progresses the mechanics of the wrist become altered, which puts abnormal stresses and wear on the joints within the wrist itself. One should be aware that not every case of this disease progresses through all stages to the severely deteriorated arthritic end-stage.
Hand therapy does not change the course of the disease; however, hand therapy can help to minimize the disability from the problem. Treatment is designed to relieve pain and restore function.
Your hand surgeon will advise you of the best treatment options and explain the risks, benefits, and side-effects of various treatments for this disease.
What can I expect?
The results of this disease and its treatment vary considerably, depending on the severity of the involvement, and whether or not the disease progresses. The disease process and response to treatment can take several months. On occasion, several forms of treatment, and even multiple operations, might be necessary.
Figure 1: Normal wristFigure 2: Wrist with Kienbocks disease and ulna that is short compared to radius
Figure 3: MRI of a wrist with Kienbocks disease showing loss of blood supply to the lunate in a patient with a short ulna
© 2006 American Society for Surgery of the Hand
When a ball or other object strikes the tip of the finger or thumb and forcibly bends it, the force tears the tendon that straightens the finger (see Figure 1a and 1b). The force of the blow may even pull away a piece of bone along with the tendon (see Figure 2). The tip of the finger or thumb no longer straightens. This condition is sometimes referred to as baseball finger.
Diagnosis
The diagnosis is evident by the appearance of the finger. Doctors will often order x-rays to see if a piece of bone pulled away and to make sure the joint is aligned.Nonsurgical Treatment
The majority of mallet finger injuries can be treated without surgery. Ice should be applied immediately and the hand should be elevated (fingers toward the ceiling.) Medical attention should be sought within a week after injury. It is especially important to seek immediate attention if there is blood beneath the nail or if the nail is detached. This may be a sign of a nail bed laceration or an open (compound) fracture.There are many different types of splints/casts for mallet fingers. The goal is to keep the fingertip straight until the tendon heals. Most of the time, a splint will be worn full-time for eight weeks (see Figure 3). Over the next three to four weeks, most patients gradually begin to wear the splint less frequently. The finger usually regains acceptable function and appearance with this treatment. Nevertheless, it is not unusual to lack some extension at the conclusion of treatment. Your surgeon or hand therapist will instruct you about how to wear the splint and will also show you exercises to maintain motion in the middle joint (the proximal interphalangeal joint) so your finger does not become stiff. Once your mallet finger has healed, your surgeon or hand therapist will teach you exercises to regain motion in the fingertip.
In children, mallet finger injuries may involve the cartilage that controls bone growth. The doctor must carefully evaluate and treat this injury in children so that the finger does not become stunted or deformed.
Surgical Treatment
(c) 2013 American Society for Surgery of the Hand
The most common medical condition causing arthritis at the joint is termed rheumatoid arthritis. Rheumatoid arthritis affects the inner coating of the joint, called the synovium, and can result in the loss of the cartilage between the joints. The cause of rheumatoid arthritis is not known.
Other conditions that can cause loss of the cartilage include previous injuries and other medical conditions such as gout, psoriasis, or infection.
The diagnosis of arthritis is confirmed by taking x-rays. Figure 3 is an x-ray of a hand with arthritis: the x-ray shows narrowing of the space between the bones, which is a sign that cartilage has been lost.
If medical treatment fails, then surgery can be considered. There are many surgical options. One option is synovectomy, which is the removal of destructive tissue. Also, since this disease can cause loosening of the tissues around the joint, these tissues can sometimes be tightened to provide relief.
If the joint is completely destroyed, then joint replacement or joint fusion are effective surgical options. The joints can be replaced with a silicone implant (silicone is a plastic like material; see Figure 4) or metal. Joint replacement is very useful, especially for older or less active individuals. Fusion—or making the joint solid—is an effective treatment of thumb MP arthritis.
Problems can occur after any type of surgery, including infection, loosening, or breakage of the artificial joint. Research is continuing to try to improve joint replacement and reconstruction in the hand.
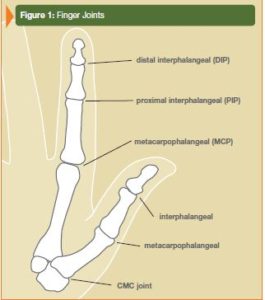
Figure 1: Finger Joints
Figure 2: Ulnar drift (fingers point towards little finger side)
Figure 3: X-ray of arthritis of the MP joint . The joint on the right has no space between the bones when compared to the joint on the left because of cartilage loss
Figure 4: X-rays of silastic finger joint replacements
© 2012 American Society for Surgery of the Hand

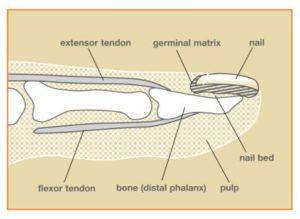
What is involved with injuries of the nail bed?
Injuries to the nail are often associated with damage to other structures that are in the same location. These include fractures of the bone (distal phalanx), and/or cuts of the nailbed, fingertip skin (pulp), tendons that straighten or bend the fingertip, and nerve endings.What causes these injuries?
Many result from crush injuries after getting the fingertip caught in a door. Any type of pinching, crushing, or sharp cut to the fingertip may result in injury to the nail bed.Presentation of injuries of the nail bed
Simple crushes of the fingertip may result in a very painful collection of blood (hematoma) under the nail. More severe injuries can result in cracking of the nail into pieces, or tearing off of pieces of the nail and/or fingertip, and possible injuries to the adjacent structures.Diagnosis of these injuries
An accurate history of the cause of the injury should be obtained. X-rays are recommended to look for associated fractures that may require treatment. The full extent of the injury may not be evident until adequate anesthesia (usually local) is given and the nail is examined with magnification. Other medical conditions that may affect healing should be discussed with your physician.Restoring the normal anatomy of the nail and surrounding structures is the goal of treatment. Simple hematomas are drained by making a small hole in the nail in order to relieve the pressure and provide pain relief. Straightforward cuts are repaired to put the parts back where they belong.
Repairing the nail bed to which the fragments of bone are attached usually restores alignment of many fractures of the fingertip. Larger fragments of bone may need to be pinned or require splinting to heal the fracture. Missing areas of nail bed can be grafted from the same finger or from other digits. Tendon injury may require splinting or pinning. Local flaps of skin may be used to replace missing skin, or the open area of skin may be allowed to just heal on its own, or covered with a skin graft.
Prognosis
The final appearance and function of the nail and surrounding structures depends on the ability to restore the normal anatomy. If the injury is sharp and can be repaired, a normal nail is likely. If there is more severe crushing of the nail bed, then there is a greater likelihood of nail bed scarring and subsequent deformity of the nail. If the germinal matrix (crescent-shaped zone at the base of the nail bed from which the nail grows) is injured, there will likely be a deformity of the nail as it grows. The function of the fingertip also depends on the extent of injury to structures other than the nail. It normally takes 3-6 months for the nail to grow from the cuticle to the tip of the finger.
Surgical Reconstruction
Loss of part or all of the nail bed can be reconstructed with grafts from other digits. Grafts may be taken from the nail bed of a toe to prevent further injury or deformity of the fingers. The most common graft is a split-thickness graft to reconstruct missing nail bed.
© 2006 American Society for Surgery of the Hand
Nerves serve as the “wires” of the body that carry information to and from the brain. Motor nerves carry messages from the brain to muscles to make the body move. Sensory nerves carry messages to the brain from different parts of the body to signal pain, pressure, and temperature. While the individual axon (nerve fiber) carries only one type of message, either motor or sensory, most nerves in the body are made up of both.
Once the nerve cover is fixed, the nerve fibers generally begin to start growing across the repair site after three or four weeks. The nerve fibers then usually grow down the empty nerve tubes up to one inch every month, depending on the patient’s age and other factors. This means that with an injury to a nerve in the arm 11 or 12 inches above the fingertips, it may take as long as a year before feeling returns to the fingertips. The feeling of pins and needles in the fingertips is common during the recovery process. While this can be uncomfortable, it usually passes and is a sign of recovery.
What is my role in recovery and what kind of results can I expect?
The patient should be aware of several things while waiting for the nerve to heal. Your doctor may recommend therapy to keep joints flexible. If the joints become stiff, they will not work even after muscles begin to work again. When a sensory nerve has been injured, the patient must be extra careful not to burn or cut their fingers since there is no feeling in the affected area. After the nerve has recovered, the brain gets “lazy,” and a procedure called sensory re-education may be needed to improve feeling to the hand or finger. Your doctor will recommend the appropriate therapy based on the nature of your injury.
Factors that may affect results after nerve repair include age, the type of wound and nerve, and location of the injury. While nerve injuries may create lasting problems for the patient, care by a physician and proper therapy help return to more normal use.
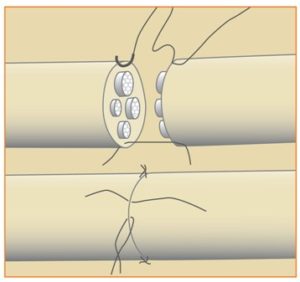
Figure 1: Nerve with bundles of individual nerve fibers and surrounding outer sheath (“insulation”)
Figure 2: Nerve repair with realignment of bundles
© 2006 American Society for Surgery of the Hand
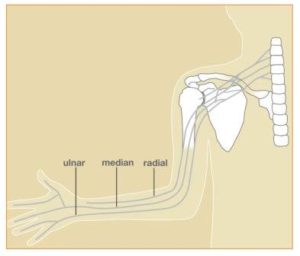
Local pressure on a nerve (“compression neuropathy”) causes numbness in distinct patterns that follow the area supplied by that nerve (see diagrams). Also, the muscles that are controlled by the compressed nerve may exhibit weakness, wasting, or twitching. The pressure may come from injury, thickened muscles, bands of connective tissue, enlarged blood vessels, ganglion cysts, or arthritic spurs. Ulnar nerve compression (see Figure 1) at the wrist causes numbness and tingling of the little finger, part of the ring finger, and the little finger side (ulnar side) of the palm. Ulnar nerve compression at the elbow causes not only the numbness noted above, but also numbness on the back of the ulnar side of the hand. Pressure on the radial nerve (see Figure 1) in the forearm or above the wrist can cause numbness over the back of the thumb, the index finger, and the web between these two digits. If the median nerve (see Figure 1) is compressed at or just below the elbow, numbness is felt not only in the same area as in CTS but also over the palm at the base of the thumb. Compression neuropathies may require surgery to release pressure on the nerve(s) to get relief.
Figure 1: Sensory distribution of nerves
Nerves in the hands and forearm have their roots in the neck. Pressure on nerves in the neck (C6-T1) (see Figure 2, 3) can be caused by numerous conditions. Arthritis may cause bone spurs or narrowing of the spinal canal, causing pressure on nerves, or degenerating discs may press directly on the nerves at the spinal column or as they leave the spinal column and pass to the upper limbs. Diseases, infections, tumors, blood vessels abnormalities, and other conditions of the spinal cord itself, in the neck, can cause pressure on the cord, which may result in numbness, tingling, or aching in the arm, forearm or hand. Weakness and/or wasting of muscles supplied by that nerve may be found. Decreased reflexes in the arm and forearm may also result from pressure on certain specific nerves in the neck. The pattern or zone of the numbness is often very distinct for each nerve root affected (see Figure 2).
Figure 2: Cervical root distribution
Figure 3: Interconnections of nerves originating in the neck
Sometimes, a nerve may suffer from pressure at more than one area. For example, a nerve may be compressed in the neck, and then again further down the arm, for example at the wrist. This is called “double crush”. When a nerve suffers from pressure at one level, it may be more susceptible to problems from pressure at another level.
Numb hands and tingling in the hands can be caused by diseases of the central nervous system. Multiple sclerosis, stroke, and other disorders of the brain and spinal cord may sometimes cause numbness in the forearm and hand.
Other diseases can affect the nerves in the upper limb, causing numbness, tingling, burning. If the symptoms are more diffuse, that is, in the hands and forearms (and in the legs and feet), the cause may be a condition called “peripheral neuropathy”. The pattern of numbness is not usually that of one nerve, but instead may be generalized, like the pattern of a glove. There may or may not be pain and the numbness is often constant. Diabetes, alcoholism, and old age are common known causes of neuropathy. Poisoning from metals and industrial compounds are also possible causes.
Certain medications, such as cancer treatment drugs, are known to cause numbness and tingling in the hands. Some of these cause temporary numbness that resolves after completion of the chemotherapy treatment. Others may cause permanent numbness. Nutritional deficiencies, such as vitamin B1 deficiency, may result in numbness and tingling.
The pattern and distribution of numbness, tingling, burning, dullness, and muscle changes help to determine if the source is pressure on a nerve at a particular level (e.g. neck, wrist, elbow), disease, medication, nutritional, or other conditions. Depending on the suspected cause, further testing, such as X-ray, MRI, nerve tests (such as EMG), or blood tests may be used to help confirm a diagnosis, and specific treatment recommendations can then be made.
(c) 2007 American Society for Surgery of the Hand. Developed by the ASSH Public Education Committee
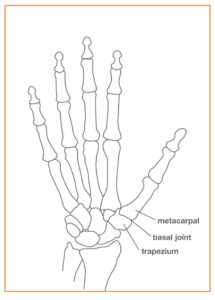
- At the base of the thumb, where the thumb and wrist come together (the trapeziometacarpal or basilar joint)
- At the joint closest to the fingertip (the distal interphalangeal or DIP joint)
- At the middle joint of a finger (the proximal interphalangeal or PIP joint)
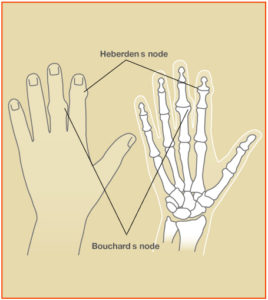
All forms of hand arthritis can cause stiffness, swelling, pain, and deformity. Osteoarthritis sometimes causes bony nodules at the middle joint of the finger (Bouchard’s nodes) or at the end joint of the finger (Heberden’s nodes) (see Figure 2). Osteoarthritis at the basilar joint can cause swelling, a bump, and a deep, aching pain at the base of the thumb. Weakness of grip and pinch can make it hard to open a jar or turn a key for those with osteoarthritis.
The Diagnosis of Osteoarthritis
When diagnosing osteoarthritis, your doctor will ask you about your hands and other joints. Explain how your symptoms affect what you do. Your doctor will check how your hands look and function. X-rays of joints with osteoarthritis can show loss of normal joint space, “bone spurs,” or other changes.
How to Treat Osteoarthritis
The goals in treating osteoarthritis are to relieve pain and restore function. Brief rest—either by changing activities or wearing a splint—can help. Soft, snug sleeves can help support a joint when rigid splints are too restrictive. Heat (for example, paraffin baths and warm compresses) can soothe the joints and help keep them mobile. It is important to keep as much finger motion and function as possible. Hand therapists can teach joint protection exercises and activity modification to help protect joints. Anti-inflammatory medication or a steroid injection into the joint can decrease pain, but neither cures osteoarthritis.
Surgery is considered when the non-surgical options above have not helped. In most cases, you will tell your doctor when you are ready for surgery. The goal is to restore as much function as possible and to minimize your pain. One type of surgery is joint fusion. The worn cartilage is removed and the bones on each side of the joint are fused together, which means that the joint will not move but it will not hurt. Another choice is joint reconstruction, where the rough joint surface is removed and either replaced with your own soft tissue or with an implant. The type of surgery depends on the joint(s) involved, your anatomy, and your activities. Your hand surgeon can help you decide which type of surgery is the best for you.
© 2012 American Society for Surgery of the Hand. Developed by the ASSH Public Education Committee
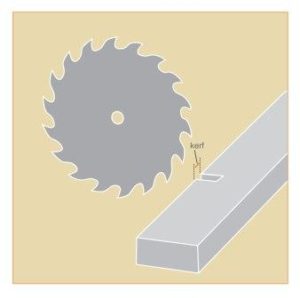
The degree of injury can vary widely. The severity depends on the location of the injury (finger, hand or forearm). Also, the depth of the injury is important (skin only vs. deeper tissues such as tendons, nerves, arteries and bone). Qualities of the saw change the injury as well. Differences in kerf (width of the cut made by the saw blade – Figure 1), tooth pattern, type and force of the saw can change the injury.
Anything that contacts the saw blade can be injured. Nerve injuries cause loss of feeling or loss of ability to control certain muscles. Circulation may be lost if the arteries are injured. Saws can also break bones. Sometimes you can lose part of the bone, which would lead to amputation. Electric shocks and burns can also occur with the operation of a power saw.
Many power saw injuries are caused by failing to follow safety precautions. Follow all the safety instructions provided for your tool. Do not override safety guards; they are there for your protection.
- Never look away from your work.
- Never use your hands to clear the scraps from a sawing worktable. Instead, use a push stick.
- Do not wear loose clothing or jewelry.
- Keep your finger off the trigger when carrying a portable power saw.
- Do not use the saw to perform a task for which it was not designed.
- Use the correct blade for the application. Set it for the correct depth to minimize the amount of exposed blade and reduce the potential for binding.
- Use sharp blades. Dull blades cause binding, stalling and possible kickback.
- Avoid cutting nails.
- Use a rip fence whenever possible.
- When starting, let the saw reach full speed before cutting and support the work firmly so it will not shift.
- If the saw stalls, switch off the power and unplug the tool before trying to restart it.
- When working with metal, secure the metal materials with clamps or in a vise to keep it from moving.
- Check for proper blade guard operation before each cut.
- When starting or stopping the saw, make sure the work is not touching the blade.
- Lower a table saw blade below the table top when finished.
- Keep a clear head, concentrate, and DO NOT DRINK ALCOHOL before using this tool!
There are now commercial table saw products available to decrease injury. The technology works quickly to stop the blade from cutting if it senses you have touched the blade.
- Stitches or bandages for cuts
- Skin grafts for larger skin injuries
- Casting for broken bones
- Amputation (removal) or replantation (reattachment) of the finger, hand or arm
Not all of these treatment options are possible. Consult your hand surgeon for the best option. Side effects such as weakness, stiffness or numbness are common after power saw injuries.
© 2014 American Society for Surgery of the Hand

Psoriasis is a skin disease in which patients have dry, red and scaly skin rashes that can occur on any part of the body. Between 5-20% of patients with psoriasis may develop an associated arthritis. Arthritis means inflamed joint. A normal joint consists of two cartilage-covered bone surfaces that glide smoothly against one another. In psoriatic arthritis, the lining of the joint—the synovium—becomes inflamed and swollen. The swollen tissues stretch supporting structures of the joints, such as ligaments and tendons. As these supporting structures stretch out, the joints become deformed and unstable. The gliding surface wears out, and joint cartilage and bone erode. In addition to the hands, this type of arthritis can affect joints in the spine, feet, and jaw.
The process of joint changes in this arthritis is very similar to the process seen in rheumatoid arthritis. The joints look red and swollen. Sometimes they feel warm. Patients have decreased motion and stiffness. While it can look very similar to rheumatoid arthritis, there are differences between the two diseases. This type of arthritis tends to:
- affect men and women equally.
- affect joints asymmetrically (What occurs in one hand may not occur in the other).
- result in red, dry, scaly skin lesions rather than distinct nodules (see Figure 1).
- swelling in the middle (PIP) joints and deformities of the end (DIP) joint of the fingers first, rather than the large finger joint (MCP joint), wrist, or over tendons.
Stiffness, swelling, and pain are symptoms common to all forms of arthritis, and sometimes it can be difficult to determine which type of arthritis you have. Findings classic for this specific type of arthritis include:
- diffusely swollen finger—sausage digit—especially the middle joint in the finger (PIP joint) (see Figure 2).
- pitting, ridging, or crumbly appearance of nails.
- deformity at the end joint (DIP) of the finger.
- dry, red, scaly skin patches which can occur anywhere, including the earlobe and hairline.
The diagnosis of this condition is made based on clinical examination, x-rays and lab tests. You will be asked questions about your symptoms and how the disease has affected your activities. It can run in families, thus your physician will ask if family members have the condition or have symptoms similar to yours. A detailed examination of your hands is important because the clinical appearance helps to clarify the type of arthritis. X-rays are also helpful. Patients with this disease often have osteolysis—loss of bone—on their x-rays. The pencil-in-cup deformity at the DIP joint is also common (see Figure 3). Other x-ray findings seen in this condition include swelling of non-bony structures, joint space narrowing, joint erosions and/or spontaneous joint fusions.These findings can occur with erosive osteoarthritis and rheumatoid arthritis as well.
There is no lab test specifically for this type of arthritis. Patients thought to have it often will have labs drawn to make sure they do not have rheumatoid arthritis or gout. Patients will often have an elevated inflammatory marker known as the sedimentation rate (ESR) but a negative rheumatoid factor (RF). Psoriasis is part of a larger group of inflammatory arthritis called spondyloarthropathies. On occasion, other lab tests may be requested to further characterize your arthritis. Sometimes a skin biopsy may be performed in a patient with hand symptoms and a skin lesion suspicious for psoriasis, without a known history of the disease.
Treatment for this arthritis aims to decrease inflammation, relieve pain, and maintain function. While there is no cure, medications are available to lessen symptoms and improve function. Optimal care involves a team approach among the patient, physicians, and therapists. The care of the psoriatic patient requires not only a hand surgeon but also a hand therapist, rheumatologist, and the patient’s primary care physician. The rheumatologist is often the physician that monitors and decides the specific type of medicine that is felt to be the most effective at that stage in the patient’s disease process.
The hand therapist will provide instruction on how to use your hands in ways to help relieve pain and protect joints. They may provide exercises, splints, wraps, and adaptive devices to help you cope with activities of daily living.This can be a progressive disease. Surgical interventions need to be appropriately timed in order to maximize function and lessen pain. Patients with psoriatic skin lesions are at increased risk for a surgical infection, so good control of the skin lesions is an important consideration when scheduling surgery.
There are many types of procedures to treat joints affected by this condition. The procedures range from joint replacements to joint fusions. The specific procedure(s) depends on many factors. These factors include the particular joint(s) involved, the degree of damage present, and the condition of surrounding joints. One of the most important factors in deciding the correct surgical procedure is the needs of the patient. There are often many ways to treat hand deformities. Your hand surgeon can help you decide on the most appropriate treatment for you.
What happens if you have no treatment?
This condition can manifest itself with different joint findings and symptoms, and these symptoms can change over time. Consequently it has been difficult to identify an individual marker for the disease. Psoriatic skin lesions do not correlate with the severity of joint involvement. Many studies show that appropriately prescribed medication can improve function and decrease pain and swelling. Studies looking at newer agents have shown delays in X-ray changes which are felt to demonstrate a slowing of the disease process. Further work is needed to understand how and to what extent medication alters the disease process.
© 2009 American Society for Surgery of the Hand. Developed by the ASSH Public Education Committee

Rheumatoid arthritis is just one type of arthritis out of many. Patients with rheumatoid arthritis often wake up with stiff and swollen joints. Early on, many patients feel tired. While this condition can affect many parts of the body, two thirds of patients with rheumatoid arthritis have wrist and hand problems. Often, the joints feel hot and look red. Rheumatoid arthritis is most common in the wrist and knuckles (Figure 1). It typically happens in both hands.
Three other common types of arthritis include:
- Wear and tear arthritis (osteoarthritis)
- Gouty arthritis
- Psoriatic arthritis
Rheumatoid arthritis affects the cells that lubricate and line joints. These tissues become swollen. They end up stretching supporting structures of the joints such as ligaments and tendons. As the support structures stretch out, the joints become deformed and unstable. The joint cartilage and bone wear away. Often the joints feel hot and look red. Rheumatoid arthritis is most common in the wrist and knuckles (Figure 1). It typically happens in both hands.
Stiffness, swelling and pain are common symptoms for all types of arthritis. There are some symptoms that are unique to rheumatoid arthritis. They are:
- Firm bumps along fingers or the elbow
- Soft lump on the back of the hand that moves as the fingers straighten
- Abnormal bend or collapse of fingers (Figure 2)
- Sudden inability to straighten or bend a finger
- A bent middle finger joint (figure 3)
- A bent end of the finger and over-extended middle joint (figure 3)
- Bones in the wrist that stick out
In addition, patients with rheumatoid arthritis often have problems with numbness and tingling in their hand (carpal tunnel syndrome). This is because the swelling of the tendons causes pressure on the nearby nerve.
How Rheumatoid Arthritis is Diagnosed
The diagnosis of rheumatoid arthritis is made based on an examination, x-rays and lab tests. Your doctor will ask questions about your symptoms and how the disease has affected your activities. Your physician will also ask whether other family members have had rheumatoid arthritis or symptoms similar to yours. There are several blood tests that are often ordered to confirm the diagnosis. MRI – a special imaging study – has also been used to help confirm the diagnosis.
Treatment for rheumatoid arthritis aims to decrease swelling, relieve pain and maintain function. While there is no cure for this condition, medications are available that slow the progression of the disease. Treatment typically involves a team approach among the patient, physicians and therapists. A rheumatologist is often the physician that monitors and determines the best type of medicine for the patient.
Your hand therapist will provide instruction on how to use your hands in ways that help relieve pain and protect joints. Therapists also can provide exercises and splints to help you live a normal life.
Rheumatoid arthritis can be a progressive disease. In certain cases, preventive surgery may be recommended. Preventative surgery may include removing lumps, removing inflamed tissue, or removing bone spurs that may rub on tendons or ligaments.
There are several types of procedures to treat joints affected by rheumatoid arthritis. This can include removal of inflamed joint lining, joint replacements and joint fusions. The specific procedure(s) chosen depends on many factors. These factors include the particular joints involved, the degree of damage present, and the condition of surrounding joints.
One of the most important factors in deciding the most appropriate surgical procedure is the needs of the patient. There are often many ways to treat hand deformities from arthritis. Your hand surgeon can help you decide on the most appropriate treatment for you.
© 2008 American Society for Surgery of the Hand
Diagnosis
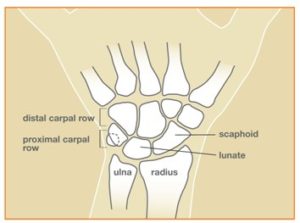
Scaphoid fractures are usually diagnosed by an x-ray of the wrist; however, x-rays do not always show scaphoid fractures. A break in the bone that cannot be seen on x-ray yet is called an “occult” fracture. If you are tender directly over the scaphoid bone (which is located in the hollow at the thumb side of the wrist as shown in Figure 2), your health care provider might recommend wearing a splint to be safe. If pain persists, a follow-up exam and x-ray in a week or two can be used to diagnose.
A CT scan, bone scan or MRI may also be used to diagnosis the fracture.
If the fracture is in a certain part of the bone or if the fracture is at all displaced (bone ends have shifted), surgery might be the best option. This might include the insertion of a screw or pins (Figure 3).
© 2014 American Society for Surgery of the Hand
A scaphoid non-union fracture refers to a wrist fracture that is failing to heal. A fracture that is healing more slowly than expected is a “delayed union” fracture.
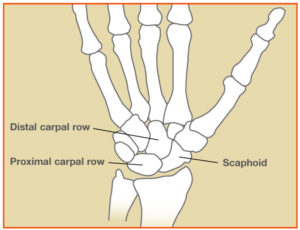
The scaphoid is one of the eight small bones in the wrist. These small bones are arranged into two rows (Figure 1). During normal wrist motion, the wrist bones move together to allow the wrist to achieve many positions that we take for granted. The scaphoid spans these two rows; in a way, it “directs” the motion of the other small bones.
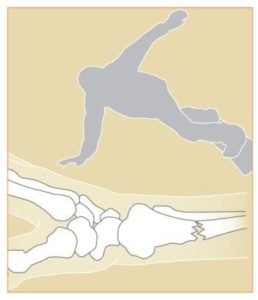
Diagnosis is confirmed most commonly with x-rays (Figures 2a and 2b). Sometimes, a CT scan and/or MRI is used to get better views of the shape and alignment of the scaphoid and assist with the diagnosis or surgery plans.
If the scaphoid fracture does not heal, you may or may not continue to have symptoms. It may be a sign that your fracture is not healing if you notice decreased strength, such as inability to do push-ups.
- Patient age
- Use of the hand
- Activity level
- Symptoms
- Tobacco use
- Other medical and/or wrist conditions
- Fracture pattern
The goals of treatment are to relieve pain, maximize function and prevent arthritis. Usually, surgery is needed to clean out the fracture site, to potentially place some form of bone graft to help bone healing, and to stabilize the fracture with pins or screws (Figure 3). Surgery options may include radial styloidectomy, proximal row carpectomy, scaphoid removal and limited wrist fusion, wrist arthroplasty or total wrist fusion.
Treatment without surgery can include use of a brace, anti-inflammatory medication or cortisone injections for pain relief. You and your hand surgeon can discuss which treatment is best for you.
© 2014 American Society for Surgery of the Hand
Skiing Injuries
One of the most common upper extremity skiing injuries is a thumb ligament tear. A ligament is the soft tissue structure that connects bones to bones. A ligament stabilizes the thumb on each side where it attaches to the hand. The ulnar collateral ligament (UCL) is on the side near the index finger. The radial collateral ligament (RCL) is on the other side (Figure 1). The UCL is the most commonly injured.
The injury typically occurs with a fall when the ski pole does not release from the hand and the pole bends the thumb in a stressful position. Three ways to avoid this injury are:
- Never place your hand down on the snow to try to avoid a fall.
- Do not place your hands through the strap, as demonstrated in Figure 2. The strap should be held alongside the pole.
- Try to let go of the pole when falling.
If your thumb hurts after a fall, it may be from a UCL injury, sometimes called “skier’s thumb.” You should visit a hand surgeon, who will determine whether it is a partial or complete ligament tear.
Treatment for Skiing Injuries
A partial tear and some complete tears can be treated with a cast or splint. Other complete tears need to be repaired surgically.
Snowboarding Injuries
Snowboarding results in injuries to the wrist and forearm. The natural protective reaction to an unexpected fall is to stop oneself. The hands are placed out to stop the fall, which can lead to a wrist injury (Figure 3). To avoid these injuries, wear wrist guards or gloves that have built-in wrist guards.
If you injure your wrist while snowboarding, visit a hand surgeon. Your doctor will examine your wrist and may use x-rays, an MRI or a CT scan to diagnose the problem.
Treatment for Snowboarding Injuries
Treatment may consist of a splint, cast or surgery. Occasionally, special devices are needed such as metal pins, plates or screws to stabilize wrist fractures and/or ligament injuries.
© 2015 American Society for Surgery of the Hand

Safety Tips
- Never put your hand or fingers near the moving parts or intake or output areas of snowblowers or lawnmowers. If there is an object in the way of any part of the machine, the machine must be turned off and the spark plug disconnected (or power cord unplugged for electric models) before attempting to remove the object. Only then should the object be removed with a tool, stick, or even a broom handle and not the hand or fingers or foot. Protect eyes from flying debris that may result.
- When being moved or picked up, snowblowers and lawnmowers should also be turned off, spark plug disconnected, and unplugged.
- Do not try to lift a machine from the bottom; even if a lawnmower is not running, the blades are sharp enough to cause serious injury.
- Wear non-slip, closed-toe shoes to prevent slipping under the machine.
- Never allow children to operate or be near the machine while in use.
Injuries
If you suffer a snowblower or lawnmower injury, seek medical attention immediately, even for seemingly small injuries.
Snowblower and lawnmower injuries may be mild or extremely severe. Small wounds or cuts can harbor unsafe bacteria. Infections are common and antibiotic medicines usually are necessary. More severe injuries can lead to multiple finger amputations. Save all body parts in a small plastic bag and place the bag on ice, then go to the closest emergency room.
Prognosis
While advances in surgery with a microscope have improved the results of replanted fingers and hands, function is never back to normal. If the fingers are too severely crushed and damaged, they might be beyond repair. Prevention is still the best treatment.© 2013 American Society for Surgery of the Hand

A variety of problems can cause hand stiffness, limiting the use and function that we often take for granted. Stiffness can occur when there are problems within and around the structures of a joint, including ligaments and muscles. Some of these problems may include:
- Arthritis
- Fractures
- Dislocations
- Bad sprains
- Tendon and muscle injuries
Evaluating Hand Stiffness
Your doctor will ask when the stiffness began and how it has progressed, including its effect on use of the hand, any injuries, other medical conditions and any prior treatment. Careful examination is performed to check the range of motion, assess swelling and tenderness, and evaluate muscles and tendons.
X-rays are usually taken to evaluate for arthritis and any other distortion of the bones and joints. For special situations, other tests may be considered such as an MRI or CT scan.
Your hand surgeon will help you decide the best approach for your individual situation. Success depends on the combined efforts of the surgeon, therapist and patient.
© 2014 American Society for Surgery of the Hand

Dactylitis
This case of dactylitis was associated with psoriatic arthritis. In this photo, the swelling extends from the palm to include the ring finger out to the small joint. Stiffness is common. There also may be pain. This swelling may be improved with medicines for the problem causing it.
Mucous Cyst
This type of cyst is called a mucous cyst. If the skin becomes thin, the cyst may break resulting in drainage of a clear sticky fluid. The resulting break in the skin may allow bacteria to reach the nearby joint, causing a joint or bone infection.
Red Dots
The small red dots seen above are in the thin part of the skin around the nail. They may also occur in the thicker pink part. This has been seen in dermatomyositis, systemic lupus, and scleroderma.
Leukonychia
Leukonychia can be seen with viral infections, intestinal and kidney diseases, poisoning, and medicines. The nail may come loose from the nail bed because of fungal infections or other causes.
Red Streaks
Red streaks seen in the fingernail area can be due to hemorrhage (bleeding). These are called splinter hemorrhages and have been seen in endocarditis (heart infection), although also reported in psoriasis, and trichinosis.
Psoriasis
Psoriasis commonly affects the nail and nailbed. Pits in the nail, loosening, blood streaks beneath the nail, and other changes may occur. A psoriasis skin patch is seen in the middle.
“Pincer” Nail
This “Pincer” nail with an abnormal side-to-side shape curve can be seen at birth or simply due to aging. However, it can also be caused by changes in the bone beneath because of disease (gout in this case).

Many different conditions can be treated by this procedure. It is necessary when a certain muscle function is lost because of a nerve injury. If a nerve is injured and cannot be repaired, then the nerve no longer sends signals to certain muscles. Those muscles are paralyzed and their muscle function is lost. This surgery can be used to attempt to replace that function. Common nerve injuries that are treated with this procedure are spinal cord, radial nerve, ulnar nerve, or median nerve injury.
Such surgery may also be necessary when a muscle has ruptured or been lacerated and cannot be repaired. Common muscle or tendon injuries that are treated with this surgery are tendon ruptures due to rheumatoid arthritis or fractures and tendon lacerations that cannot be repaired after injury.
This surgery may also be needed if a muscle function has been lost due to a disorder of the nervous system. In this situation, the nervous system disease or injury prevents normal nerve signals from being sent to a muscle, and imbalance in hand function occurs. The muscle imbalance or muscle loss due to nervous system disease may be treated with tendon transfers. Common nervous system disorders treated with this surgery are cerebral palsy, stroke, traumatic brain injuries, and spinal muscle atrophy.
Finally, there are some conditions in which babies are born without certain muscle functions. In these situations, the missing muscle functions can sometimes be treated with this procedure. Common conditions treated this way include hypoplastic (underdeveloped) thumbs and birth brachial plexopathy (nerve problem with paralysis).
Procedure
Below the elbow, there are over forty muscles. Each different muscle has a different function. For example, there are 9 muscles that move the thumb. Each muscle has a starting point (origin), and tapers down from its muscle belly into a tendon that then attaches onto bone (insertion) in a specific place; when the muscle fires (contracts), it causes a certain motion (action).During this surgery, the origin of the muscle is left in place; the nerve supply and blood supply to the muscle is left in place. The tendon insertion (attachment) onto bone is detached and re-sewn into a different place. It can be sewn into a different bone, or it can be sewn into a different tendon. After its insertion has been moved, when the muscle fires, it will produce a different action, depending on where it has been inserted.
Alternatives
You can discuss other treatment choices with your hand surgeon. Other options may include repairing the nerve that has been injured, or repairing the tendon or muscle that has been injured. In some cases, tendon grafts can be used, in which a portion of intact tendon is removed, without its muscle, and used to bridge a gap in an injured tendon. In other cases, tendon lengthening or bone fusions may be necessary as part of reconstructing hand function.Risks
All surgery has some risk, although those risks may be small. All surgeries produce a surgical scar. Surgical incisions may develop infection. All surgeries require the use of anesthesia, and will require a complete history and physical examination by your primary care physician to determine if you have medical risks associated with anesthesia. Evaluation by the anesthesiologist will help outline your risks and options.When a tendon is transferred and sewn into another position, the tendon transfer will need a period of time to heal, usually about one to two months. A splint or cast may be used, followed by therapy to teach you the new tendon function. Finally, exercises will be needed to strengthen the muscle after your hand surgeon feels the tendon transfer has sufficiently healed. You will need to follow post-operative instructions. Movement too early can lead to rupture of the tendon transfer. Movement too late can lead to excessive scarring of the tendon with resultant stiffness. Discussion of your individual case with your hand surgeon will help you further understand the risks and benefits associated with this surgery.
Example
After a fracture of the wrist, the fragments of bone associated with the fracture may erode the tendon that straightens the tip of the thumb. In this situation, the thumb tip would not be able to move upward (extend). The muscle that extends the tip of the thumb is the extensor pollicus longus (EPL) (see Figure 1). In this example, the EPL tendon typically cannot be directly repaired because it is too frayed. There are two muscles that extend the index finger. Just like the body has two kidneys, so that one can be spared if necessary, the body also has two tendons that extend the index finger. One tendon is left intact on the index finger so that it won’t lose extension, and the “extra” tendon can be transferred over to the thumb to replace the lost function. The tendon insertion of the “extra” index finger extensor tendon (Extensor indicus proprius—EIP) is detached. The EIP tendon is then re-directed and sewn into the thumb bone or thumb tendon (EPL).After this type of surgery, a splint or cast is used for one month, after which supervised therapy may be started to re-learn how to use the transferred tendon to extend the thumb. Gentle movement with a protective splint may be used for an additional month. If adequate progress is made, the therapy may be advanced one month later to re-learn activities and to strengthen the muscle, with restoration of the ability to extend the thumb. A supervised hand therapy program for retraining the muscles is extremely important to achieve the best possible function.
© 2011 American Society for Surgery of the Hand. Developed by the ASSH Public Education Committee

Trauma – A direct blow to the elbow may result in swelling of the tendon that can lead to degeneration. A sudden extreme action, force, or activity could also injure the tendon.
Who gets tennis elbow/lateral epicondylitis?
The most common age group that this condition affects is between 30 to 50 years old, but it may occur in younger and older age groups, and in both men and women.
Activity modification – Initially, the activity causing the condition should be limited. Limiting the aggravating activity, not total rest, is recommended. Modifying grips or techniques, such as use of a different size racket and/or use of 2-handed backhands in tennis, may relieve the problem.
Medication – anti-inflammatory medications may help alleviate the pain.
Brace – a tennis elbow brace, a band worn over the muscle of the forearm, just below the elbow, can reduce the tension on the tendon and allow it to heal.
Physical Therapy – may be helpful, providing stretching and/or strengthening exercises. Modalities such as ultrasound or heat treatments may be helpful.
Steroid injections – A steroid is a strong anti-inflammatory medication that can be injected into the area. No more than (3) injections should be given.
Shockwave treatment – A new type of treatment, available in the office setting, has shown some success in 50–60% of patients. This is a shock wave delivered to the affected area around the elbow, which can be used as a last resort prior to the consideration of surgery.
Surgery
Surgery is only considered when the pain is incapacitating and has not responded to conservative care, and symptoms have lasted more than six months. Surgery involves removing the diseased, degenerated tendon tissue. Two surgical approaches are available; traditional open surgery (incision), and arthroscopy—a procedure performed with instruments inserted into the joint through small incisions. Both options are performed in the outpatient setting.
Recovery
Recovery from surgery includes physical therapy to regain motion of the arm. A strengthening program will be necessary in order to return to prior activities. Recovery can be expected to take 4–6 months.
Figure 1: The muscle involved in this condition, the extensor carpi radialis brevis, helps to extend and stabilize the wrist
© 2006 American Society for Surgery of the Hand
Trauma – A direct blow to the elbow may result in swelling of the tendon that can lead to degeneration. A sudden extreme action, force, or activity could also injure the tendon.
Who gets tennis elbow/lateral epicondylitis?
The most common age group that this condition affects is between 30 to 50 years old, but it may occur in younger and older age groups, and in both men and women.
Activity modification – Initially, the activity causing the condition should be limited. Limiting the aggravating activity, not total rest, is recommended. Modifying grips or techniques, such as use of a different size racket and/or use of 2-handed backhands in tennis, may relieve the problem.
Medication – anti-inflammatory medications may help alleviate the pain.
Brace – a tennis elbow brace, a band worn over the muscle of the forearm, just below the elbow, can reduce the tension on the tendon and allow it to heal.
Physical Therapy – may be helpful, providing stretching and/or strengthening exercises. Modalities such as ultrasound or heat treatments may be helpful.
Steroid injections – A steroid is a strong anti-inflammatory medication that can be injected into the area. No more than (3) injections should be given.
Shockwave treatment – A new type of treatment, available in the office setting, has shown some success in 50–60% of patients. This is a shock wave delivered to the affected area around the elbow, which can be used as a last resort prior to the consideration of surgery.
Surgery
Surgery is only considered when the pain is incapacitating and has not responded to conservative care, and symptoms have lasted more than six months. Surgery involves removing the diseased, degenerated tendon tissue. Two surgical approaches are available; traditional open surgery (incision), and arthroscopy—a procedure performed with instruments inserted into the joint through small incisions. Both options are performed in the outpatient setting.
Recovery
Recovery from surgery includes physical therapy to regain motion of the arm. A strengthening program will be necessary in order to return to prior activities. Recovery can be expected to take 4–6 months.
Figure 1: The muscle involved in this condition, the extensor carpi radialis brevis, helps to extend and stabilize the wrist
© 2006 American Society for Surgery of the Hand

Thumb arthritis is a genetic predisposition: like graying and thinning of the hair, it comes with age and it shows up earlier in some families. Unlike thinning of the hair, women tend to get thumb arthritis sooner than men do.
Patients with thumb arthritis report pain and weakness with pinching and grasping. For instance, opening jars, turning doorknobs or keys, and writing are often painful.
The diagnosis is made by talking with you and examining you. The appearance of the thumb can change with the development of bone spurs and stretching of soft tissues (ligaments) (see Figure 2). A grinding sensation may also be present at the joint (see Figure 3). X-rays are not necessary to make the diagnosis, but they can help you understand the disease and they can help when surgery is being considered.
Surgery consists of removing the joint either by removing a bone or connecting the bones together. There are options for moving one of your tendons to secure or cushion the bone, and each hand surgeon has a different opinion on whether this is helpful (see Figure 4). After surgery, a splint or cast is worn for several weeks.
(c) 2013 American Society for Surgery of the Hand
Developed by the ASSH Public Education Committee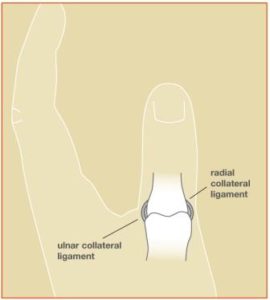
The most common ligament to be injured in the thumb is the ulnar collateral ligament. This helps connect the thumb to the hand on the side near the index finger. It allows the thumb to act like a post. Injury to this ligament is sometimes called “skier’s thumb” because it is a common injury from a ski pole. The radial collateral ligament is on the other side of the thumb. It can tear, but this is not as common as a tear on the ulnar side. See Figure 1 to view both ligaments.
If the injury is chronic, the ligament might not be able to heal even with treatment. In these cases, a new ligament sometimes is created using a tendon. If there is arthritis at the joint, fusing the joint so that it does not move at all might be the best option.
Figure 1: The ulnar collateral ligament (UCL) and the radial collateral ligament (RCL) help stabilize the thumb.
Figure 2: Upon falling, the ski pole may bend the thumb in an extreme position and tear the ulnar collateral ligament (UCL), the so-called “skier’s thumb” injury.
© 2015 American Society for Surgery of the Hand
Stenosing tenosynovitis is a condition commonly known as “trigger finger.” It is sometimes also called “trigger thumb.” The tendons that bend the fingers glide easily with the help of pulleys. These pulleys hold the tendons close to the bone. This is similar to how a line is held on a fishing rod (Figure 1). Trigger finger occurs when the pulley becomes too thick, so the tendon cannot glide easily through it (Figure 2).
- Pain
- Popping
- Catching feeling
- Limited finger movement
Common treatments include, but are not limited to:
- Night splints
- Anti-inflammatory medication
- Changing your activity
- Steroid injection
If non-surgical treatments do not relieve the symptoms, surgery may be recommended. The goal of surgery is to open the pulley at the base of the finger so that the tendon can glide more freely. The clicking or popping goes away first. Finger motion can return quickly, or there can be some stiffness after surgery. Occasionally, hand therapy is required after surgery to regain better use.
© 2015 American Society for Surgery of the Hand
Warts are bumps on the skin and may feel rough to the touch. The technical name is verruca vulgaris. They appear in areas of skin that grow faster than normal due to a virus called human papilloma virus (HPV). They can spread, and some people can more easily get them. There is no cure for the HPV virus. Most people will naturally fight off the virus from their body within 2-3 years of getting it. However, it can come back. These bumps on hands can be uncomfortable and embarrassing to have, but are not cancerous.
The bumps can be very itchy, can bleed if irritated, and the skin around them can become uncomfortable. If on fingers, they are sometimes confused with other problems such as fluid filled sacs (cysts) or bone spurs from arthritis.
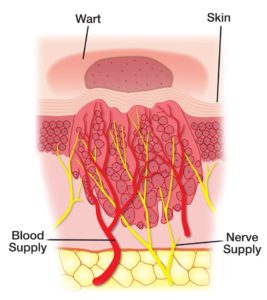
A primary care physician or dermatologist are often the first physicians to treat this problem. There are many different treatment options. While it is very rare, it is important to know that a bump that does not respond to regular treatment can be a sign of a developing skin cancer lesion.
Treatments include simple solutions such as placing duct tape over the bump after rubbing it with a pumice stone. Other methods may include applying salicylic acid or liquid nitrogen to freeze the bump. If these methods do not work, a chemical called cantharidin may be used. Finally, surgical excision or biopsy might be indicated for bumps that do not seem to go away or are in areas that are hard to treat with other methods.
Perhaps the most important thing to remember during treatment is patience. Tried and true treatments generally work but take time.
© 2013 American Society for Surgery of the Hand
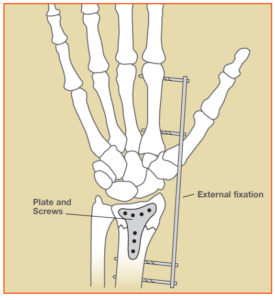
Some wrist fractures are stable. “Non-displaced” breaks, in which the bones do not move out of place initially, can be stable. Some “displaced” breaks (which need to be put back into the right place, called “reduction” or “setting”) also can be stable enough to treat in a cast or splint. Other fractures are unstable. In unstable fractures, even if the bones are put back into position and a cast is placed, the bone pieces tend to move or shift into a bad position before they solidly heal. This can make the wrist appear crooked.
Some fractures are more severe than others. Fractures that break apart the smooth joint surface or fractures that shatter into many pieces (comminuted fractures) may make the bone unstable. These severe types of fractures often require surgery to restore and hold their alignment. An open fracture occurs when a fragment of bone breaks and is forced out through the skin. This can cause an increased risk of infection in the bone.
Diagnosis
Your hand surgeon will do a physical examination and obtain x-rays to see if there is a broken bone. Sometimes, tests such as a CT scan or MRI scan may be needed to get better detail of the fracture fragments and other injuries. Ligaments (the soft tissues that hold the bones together), tendons, muscles and nerves may also be injured when the wrist is broken. These injuries may need to be treated also.
- Type of fracture, whether it is displaced, unstable or open
- Your age, job, hobbies, activity level, and whether it is your “dominant” hand
- Your overall general health
- Presence of other injuries
A padded splint might be worn at first in order to align the bones and support the wrist to provide some relief from the initial pain. If the fracture is not too unstable, a cast may be used to hold a fracture that has been set. Other fractures may benefit from surgery to put the broken bones back together and hold them in correct place.
Fractures may be fixed with many devices. Pins, screws, plates, rods or external fixation can all be used (Figure 2). A small camera might be used to help visualize the joint from the inside. Sometimes the bone is so severely crushed that there is a gap in the bone once it has been realigned. In these cases, a bone graft may be added to help the healing process. Your hand surgeon will discuss the options that are best for your healing and recovery.
Recovery
During recovery, it is very important to keep your fingers moving to keep them from getting stiff. Your hand surgeon will have you start moving your wrist at the right time for your fracture. Hand therapy is often helpful to recover motion, strength and function.
Recovery time varies and depends on a lot of factors. It is not unusual for recovery to take months. Even then, some patients may have stiffness or aching. Severe wrist fractures can result in arthritis in the joint. Occasionally, additional treatment or surgery is needed.
Figure 1: Wrist bones shown with a non-displaced fracture of the radius.
Figure 2: Radius fracture shown stabilized with external fixation and plate and screws.
© 2015 American Society for Surgery of the Hand.

The most common ligament to be injured in the wrist is the scapho-lunate ligament (see Figure 2). It is the ligament between two of the small bones in the wrist, the scaphoid bone and the lunate bone. There are many other ligaments in the wrist, but they are less frequently injured. Sprains can have a wide range of severity; minor sprains may have minimal stretch of the ligaments, and more severe sprains may represent complete tears of the ligament(s). Another common ligament injured is the TFCC (triangular fibrocartilage complex).
Diagnosis
Initially your doctor will examine your wrist to see where it hurts and to check how it moves. X-rays are taken to make sure there are no broken bones or dislocated joints (see Figure 3). Occasionally other studies, such as Magnetic Resonance Imaging (MRI), may be performed.Treatment
Chronic injuries
The term “chronic” refers to an old injury of greater than several months to years. If there is no or minimal cartilage damage, the ligament may be reconstructed. If there is moderate to severe cartilage damage (arthritis), symptoms may include pain, stiffness, and swelling. Chronic injuries may first be treated with splinting and non-steroidal anti-inflammatory medicines, and later with cortisone injections. If these treatments fail, surgery may be an option. Various types of procedures are possible, including a partial wrist fusion, removal of arthritic bones (“proximal row carpectomy”), wrist replacement, or complete wrist fusion. Your doctor will determine the best course of treatment.Associated injuries
Future treatments
Prognosis
© 2013 American Society for Surgery of the Hand
 — Logo")
 — Logo")
 — Logo")