PATIENT RESOURCES
Procedures and Treatment
Common procedures we do:
Cortisone is a steroid normally produced by your body, and it is a powerful anti-inflammatory. Corticosteroids tend to shrink, thin and slow things down. These steroids are different from anabolic steroids, which have been abused by athletes to build muscle and enhance performance.
Results
The injection should take effect within a few days, and the benefits can last for many weeks; however, results are not the same for everyone or every problem. For some conditions, one injection solves the problem. For others, several injections may be required. There is no set rule as to how many injections a person can get. Your doctor might limit the number of injections because repeated cortisone can damage tendons and/or cartilage.Side Effects
The most common side effect of steroid injections is known as a “flare.” This pain is felt for one or two days after the injection. It can be treated with ice and by resting the area injected.Other side effects might include:
- A rise in blood sugar level for diabetic patients for about five days
- Thinning of the skin
- “Lightening” of the skin at injection site (more common in patients with dark skin)
- Weakening of tendons, making them more likely to rupture
- Allergic reactions (rare)
One of the rare but more serious problems is an infection, especially if the injection was given into a joint. If you notice redness, extreme pain or heat at the injection site, or if you have a fever greater than 101° after an injection, you should call your doctor.
© 2015 American Society for Surgery of the Hand

Other Procedures and Treatments:

Surgery
When an operation is necessary, the surgeon removes the injured body part. Prior to surgery, the surgeon will do a careful examination of your hand. Often the surgeon will obtain x-rays or other imaging studies to assess the damage to your finger/hand. The area removed is based on the extent of the injury and the health of the remaining body part. In many cases, the surgeon is able to close the site of the surgery by rearranging skin and shortening bone or tendon. Sometimes, the surgeon may have to use skin, muscle or tendons from another part of your body to close the site of the surgery. In most finger tip injuries, the surgeon is able to close the site directly. In more extensive injuries, the surgeon may shape the finger or the hand to be able fit a prosthesis later.
For the first couple of weeks, you should expect some pain. Pain will be controlled with pain medications. While you are healing, your doctor will tell you how to bandage and care for the surgical site and when to return to the office for follow-up care. You may be given exercises to build your strength and flexibility. You may be asked to touch and move your skin to desensitize it and keep it mobile.
Prosthesis
A prosthesis is made from an impression cast taken from the residual finger or limb and the corresponding part on the undamaged hand. This process can create an exact match to the details of the entire hand. The finger or hand prosthesis is made from of a flexible, transparent silicone rubber. The colors in the silicone are carefully matched to your skin tones to give the prosthesis the life-like look and texture of real skin. It is usually held on by suction, and the flexibility of the silicone permits good range of motion of the remaining body parts. Fingernails can be individually colored to match almost perfectly. The nails can be polished with any nail polish, and the polish can be removed with a gentle-action nail polish remover. Silicones are resistant to staining, so inks wash off easily with alcohol or soap and warm water. With proper care, silicone prosthesis may last 3-5 years. Usually, three months after you are completely healed from surgery and all swelling has subsided, creation of your prosthesis can begin. You may need therapy to learn to use your new prosthesis.
Emotional Recovery
The loss of a body part, especially one as visible as a finger or hand, can be emotionally upsetting. It may take time to adapt to changes in your appearance and your ability to function. Talking about these feelings with your doctor or other patients who have had this condition often helps you come to terms with your loss. You may ask your doctor to recommend a counselor to assist with this process. It is important to remember that with time, you will adapt to your situation by finding new ways of doing your daily activities. The Amputee Coalition of America www.amputee-coalition.org/index.html is another helpful resource. These resources can help you to be strong during the course of recovery. Remember that quality of life is directly related to attitude and expectations – not just obtaining and using a prosthesis.
© 2011 American Society for Surgery of the Hand.
DESCRIPTION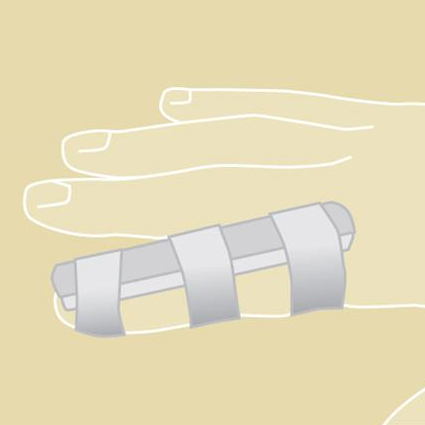
Splints and casts are supports that are used to protect injured bones and soft tissues. A cast completely encircles the limb with a hard, rigid outer shell (Figures 1 and 2). A splint provides rigid support along just the side(s) of the limb, with soft or open areas in between (Figures 3 and 4). Splints are often used in the immediate post-operative or injury phase, when there is a greater chance of swelling. A splint can better allow for swelling. Your doctor will decide which type of support is most appropriate for you and your arm condition.
MATERIALS
Casts are made with plaster or ‘fiberglass’ to form the hard supportive layer, and a soft lining of cotton or similar material for padding. Fiberglass is lighter, more durable, and “breathes” better than plaster. Plaster is less expensive and shapes better than fiberglass for some uses. Both materials come in strips and rolls, and are dipped in water to start the setting process. Most casts have a layer of padding underneath the hard material. X-rays can be taken through casts, but they do block some of the x-ray detail.
Splints can be made with these same materials or with plastic, fabric, or padded aluminum. They can be custom-made, or they may be pre-made. They come in a variety of shapes and sizes, depending on the specific need. They often have Velcro straps, which makes them easier to take on and off.
For fiberglass casts, water compatible padding does exist; ask your doctor if they have it available. Not all injuries can be treated with a waterproof cast. Waterproof casts can be submerged. It is best to avoid water from lakes, rivers and oceans when wearing a waterproof cast because your skin can become irritated if dirt or sand gets inside the cast. When you come in contact with chlorinated water or dirty water, rinse the cast with fresh water when you are done swimming. Allow the inside of the cast to drain as much as possible after it gets wet. If you have a cast that goes past your elbow, be sure to drain the area around the elbow well. The rest of the water will evaporate. Sweat will not harm the cast liner, but consider rinsing the cast with clean water after excessive sweating.
SIGNS AND SYMPTOMS
Swelling due to your injury or surgery is usually worst during the first 2 or 3 days. Swelling can cause pressure in your splint or cast, making it feel tighter. To help avoid or reduce swelling, you should put your hand and arm above your heart by propping it up on pillows or some other support if possible. Elevation helps gravity to drain the blood and fluid that causes swelling out of your hand and arm. This can also decrease pain. If swelling increases too much, a cast or splint can become too tight.
The following signs and symptoms should be watched for, and if they occur, you should contact your doctor promptly for advice:
•Worsening pain
•Numbness and tingling in your hand or fingers, which may indicate excessive pressure on the nerves
•Burning and stinging, which may result from too much pressure on the skin
•Excessive swelling of the hand, which may mean the veins are being blocked
•Loss of active movement of your fingers, which may indicate muscle damage
•Sometimes a cast may need to be changed if the cast is too tight or if it gets too loose when the swelling goes down
TREATMENT – CAST AND SPLINT CARE
Keep your cast or splint clean and dry. Being in contact with damp padding can irritate your skin. Plaster gets softer and weaker when it gets wet. Use plastic bags or a waterproof cast cover to keep your splint or cast dry when bathing. Seal the bag with tape or rubber bands. Elevate your hand in the shower above your head, because otherwise water can still run under the seal and into your cast. Do not keep it constantly covered because moisture may build up from normal sweating.
Do not let dirt, sand, or other materials get inside of your splint or cast. If you feel itching, do not place anything inside your cast because you can injure your skin; ask your doctor for advice. Never trim the cast or splint by yourself. If there are rough edges or if your skin gets irritated around the edges of the cast, notify your doctor, who has the proper tools to fix it. If the cast or splint develops cracks or soft spots, contact your doctor to see if it needs to be repaired or changed.
CAST REMOVAL
Never try to remove a cast yourself; you may cut your skin or prevent proper healing of your injury. A cast should be removed only by a professional with the proper tools and training. Casts are removed with a special type of saw that will not cut your skin.
Remember, a cast is there to protect you while your injury heals. It is only a temporary inconvenience, with the goal of helping you recover.
© 2012 American Society for Surgery of the Hand
There are several types of anesthesia for patients undergoing hand surgery. These include local, regional or general. The type used depends on the type and length of the surgery, the patient’s health and medical conditions, and preferences of the patient, surgeon, and anesthesiologist.
The numbing medications used in regional can provide between one and 24 hours of pain relief, depending on the medication used. Some local anesthetics may last as long as three days.
General Anesthesia
The patient is unconscious and does not feel anything during the surgery. The patient may receive the medicine by breathing it in or through an intravenous (IV) line.
Local Anesthesia
This typically means anesthetics for a small area. Numbing medicine is injected at the site of surgery. The patient is wide-awake during the surgery and can fully cooperate with any instructions from the surgeon, such as to move the hand or fingers. It contains medicine to stop excessive bleeding and to minimize pain in the operated area. Other medications to help you relax can also be given with this type of anesthesia. The relaxing medications are typically given through an IV line.
Regional Anesthesia
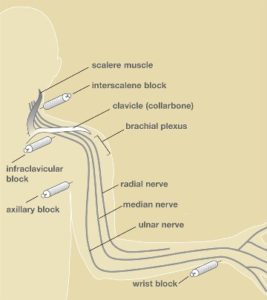
Parts of the body are put to sleep by injecting numbing medicine through a needle placed along the path of nerves. This may be around the collarbone or neck, under the arm, at the wrist, in the palm, around your finger, or through an IV in your arm. As with local anesthesia, the anesthesiologist or nurse anesthetist may add relaxing medication given through an IV line.
The injection of numbing medicine with a needle can be slightly uncomfortable or painful, but you will have IV medication to help you relax and feel comfortable during the injection. Sometimes, the anesthesiologist may use a needle connected to a nerve stimulator to precisely locate the nerve. This causes the arm or hand muscles to twitch and move, which is not painful, although it can feel strange.
Some proven advantages of this type include less need for pain medicine after surgery, faster recovery, less nausea, and, for some surgeries, less blood loss and lower risk of blood clots.
Will I be Awake During Surgery?
Some patients prefer to be awake during surgery. Others prefer to be asleep. During your surgery you can be awake or asleep, depending on what you and the surgical team decide. You will not be able to see the surgery itself because a large sterile drape is placed between you and the surgeon. This is to protect the “sterile field,” the important area of your surgery, from any contamination of germs that can cause infection.
What Are the Risks?
Some risks associated with regional or local anesthesia include pain, soreness or bruising at the needle site, or tingling that lasts for several days. Serious complications can occur, such as bleeding, infection or nerve injury, but these are very rare. Your surgeon and anesthesiologist will check to make sure you are comfortable before, during and after the procedure. Do not hesitate to tell them if you are not.
© 2014 American Society for Surgery of the Hand

Patients who are candidates for hand therapy may have been affected by an accident or trauma leaving them with wounds, scars, burns, injured tendons or nerves, fractures, or even amputations of the fingers, hands or arms. Others include patients who suffer from conditions such as carpal tunnel syndrome and tennis elbow, as well as from chronic problems such as arthritis or a neurologic condition (i.e. stroke).
What Does Hand Therapy Provide?
- Treatments without an operation
- Help with recent or long-lasting pain
- Help to reduce sensitivity from nerve problems
- Learning to feel again after a nerve injury
- Learning home exercise programs to help with movement and strength
- How to make splints to help prevent or improve stiffness (Figure 1)
- Learning to complete everyday activities with special tools
- Help getting back to work
If surgery is needed, hand therapists can also help with a patient’s recovery. This may include assistance with helping wounds heal, preventing infection, scar management and reducing swelling.
Getting Back to Work
Hand therapists are able to talk with employers about preventing problems for workers with hand or arm symptoms. They may recommend changes at your place of work or different ways of doing your job to help ensure a healthy style of work.
Find a Hand Therapist
Search for a hand therapist in your area by going to www.asht.org, the official website of the American Society of Hand Therapists.
© 2014 American Society for Surgery of the Hand. Content provided by the American Society of Hand Therapists.

- Recent injuries (bruises or fractures) or chronic injuries
- Swelling
- Stiffness
- Irritation
Benefits of Heat Treatments
Heat or warmth will help get things moving by speeding up the molecules in tissues and increasing blood flow. Heat is helpful for stiff joints and muscles, and can be useful prior to an activity. We often see an athlete warming up before a workout.
A warm shower or bath can help sore, stiff joints, especially in the early morning. A warm compress or heating pad can also relieve stiffness (Figure 1); however, too much heat could cause fainting, swelling, or burns to skin and tissues, so use heat treatments with moderation.
Benefits of Ice Treatments
If there is pain, swelling and irritation after an activity, ice treatments can reduce these symptoms. Cold slows down the molecules in tissues and reduces blood flow.
The most common cold treatments are ice or something that has been made cold by placing it in the freezer, such as a gel pack (Figure 2). Apply ice for 15 minutes, then allow a 15-minute rest before reapplying.
As with heat, too much cold can slow down and stiffen sore joints, so use this treatment with moderation. Applying ice or anything extremely cold to bare skin can cause injury. Always wrap the source of cold in some sort of fabric. If a bandage or splint is too thick and the cold is not getting through, apply the cold near the area on exposed skin. Stop using ice if you feel extreme pain or numbness due to the cold.
Special Treatments
Some special and more advanced heat or ice treatments may be used under the supervision of a therapist or physician. Some options may include:
- Therapeutic ultrasound: A qualified therapist will use ultrasound to slowly heat deeper tissues to help motion.
- Contrast bath: This is a bath that involves alternating heat and cold.
- Paraffin or warm wax: This can be used to apply heat via machines that are highly regulated and use a wax mixture that avoids skin burns.
Use caution when implementing ice or heat treatments. Monitor time and the condition of your skin, and always test the hot or cold item before applying. Contact your physician or therapist for assistance.
© 2014 American Society for Surgery of the Hand
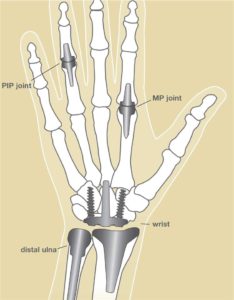
Artificial joints in the hand may help:
- Reduce joint pain
- Restore or maintain joint motion
- Improve the look and alignment of the joint(s)
- Improve overall hand function
Causes
In a normal joint, bones have a smooth surface made of a substance called articular cartilage on their ends that allows one bone to glide easily against another. Joints are lubricated by a thin layer of fluid (synovial fluid) that acts like oil in an engine to keep parts gliding smoothly. When the articular cartilage wears out, is damaged, or the joint fluid is abnormal, problems develop, and joints often become stiff and painful. This is arthritis, which may be possible to treat with this procedure.
Recovery
Therapy supervised by a trained hand therapist is almost always required after any joint replace-ment surgery, usually for several months. Special splints are generally used depending on which joint was replaced and how the surgery was done (Figure 2).
To ensure the best results after surgery, follow your surgeon and therapists’ directions, call your surgeon if you experience a sudden increase in pain or swelling, and call your surgeon if your hand or wrist becomes red, hot or crooked.
Call your surgeon or therapist if you have specific questions about your new joint(s).
Risks
Some risks of this procedure include:
- Implant loosening, fracturing or wearing down over time, which may require subsequent surgery
- Infection
- Joint stiffness or pain if the procedure or implant fails
- Dislocation of the artificial joint
- Damage to vessels, nerves or other structures in the region of the surgery
Alternatives
Some alternate procedures for treating arthritis include:
- Joint injections
- Oral medications such as aspirin or anti-inflammatory medicines
- Hand therapy exercises and protective splints
- Arthrodesis surgery to fuse bones together, which relieves pain by eliminating motion be-tween damaged joint surfaces
- Resection arthroplasty, which is a surgery to remove arthritic surfaces and/or bone
- Surgery on tendons or ligaments to repair related joint injuries
© 2014 American Society for Surgery of the Hand

Misuse: A large and growing problem
Over the last 15 years, the prescription of this medication has increased tenfold. Misuse now kills more than 100 people each day in the United States. It is responsible for more deaths than both suicide and motor vehicle collisions combined. According to the Food and Drug Administration (FDA), nearly 16,000 Americans died from overdoses involving these pain relievers in 2009. Most of these deaths were accidental.
The pain dilemma
Pain is expected after injury or surgery, and mindset matters. Pain relievers cannot take pain away; they just make the pain less bothersome. Patients quickly develop tolerance to these drugs, which means it requires more medicine to achieve the same amount of pain relief as time goes by. This is why such pain relievers work well in the short term, but do not work for long-term chronic pain.
Recreational use
These pain relievers are sometimes used by patients or their friends to get high. Over half of the teens abusing these medicines get them from family or friends without their knowledge. In addition to potential poisoning, recreational use creates addiction. One study of heroin users found that 39% of addicts reported being “hooked” on prescription pain relievers first.
The most common side effects of these drugs are nausea, constipation, itching and drowsiness. The most serious effect is a decrease in breathing, which can result in death. The chance of death can increase when pain relievers are used together with alcohol or other drugs that make you sleepy.
The progress of your treatment and your medication needs should be discussed with your providers, including your surgeon, physician assistant and nurse. While your providers want to limit pain following surgery or injury, they also understand the risks of abuse, addiction and possibly death associated with the use of these medicines. To reduce these risks, your provider may suggest switching to over the counter medicines such as ibuprofen or ancedimenifin once the initial intense pain subsides.
Disposal
These pain relievers should be disposed of when they are no longer needed to treat the injury or surgery for which they were originally prescribed. Studies report that between 10% and 30% of these pain relievers sold go unused. Leftover pain medicines kept in a patient’s home increase the risk of accidental poisoning and drug abuse. These tragedies often affect family members or friends.
Many communities have organized ways to dispose of unused pain relievers. Some law enforcement agencies have drop boxes or hold designated dates to collect unused prescription medicines. Do not flush the pills down the toilet because it releases the drugs into the waterways. Water treatment facilities do not effectively remove these dissolved drugs, so contamination of drinking water is a growing concern.

A paraffin wax unit may be rented or purchased. The units are low-cost and can be purchased from a local retailer (drugstore, department store or discount store) or online.
How to Use a Paraffin Wax Unit
First, choose a place in your home where the unit can be set up according to the instructions. Pay particular attention to the safety features to prevent accidents. These units usually can remain set up and plugged in at all times, allowing the paraffin to be melted and available for use throughout the day.
When using your unit, follow these instructions:
- Wash your hands with soap and water and dry them.
- Rub lotion onto your hands: Hand lotion allows the wax to be removed easily after treatment.
- Dip your hand into the wax (Figure 1): Your fingertips should go in first. Keep your fingers separated and submerse your hand all the way past the wrist if desired.
- Remove your hand after it has been coated with wax.
- Repeat steps 3 and 4: Dip your hand 6-8 times, waiting a few seconds between each dip. This allows layers of wax to form over your hand.
- Immediately cover your hand with a plastic bag and wrap with a hand towel (Figure 2): Wait 10-15 minutes. This will create moist, deep heat for your hand.
- Remove the towel, plastic bag and cooled wax after 10-15 minutes.
- Return the wax from your hand to the paraffin unit for reuse (Figure 3).
- Proceed with exercises that have been recommended by your hand surgeon and/or hand therapist.
When the wax level of your unit is low, you can purchase additional blocks of paraffin, usually from the store of your original purchase or a local beauty supply shop.
© 2015 American Society for Surgery of the Hand

Replantation is the surgical reattachment of a finger, hand or arm that has been completely cut from a person’s body (Figure 1). The goal of this surgery is to give the patient back as much use of the injured area as possible. This procedure is recommended if the replanted part is expected to function without pain.
In some cases, a replant is not possible because the part is too damaged. If the lost part cannot or should not be reattached, your surgeon may offer to clean, smooth and cover the cut end. This is called a completion or revision amputation. In some cases, this option will give you a better and faster recovery than a replant.
Procedure
There are a number of steps in the replantation process.
- Step 1: Damaged tissue is carefully removed.
- Step 2: Bone ends are shortened and rejoined with pins, wires, or plates and screws. This holds the part in place to allow the rest of the tissues to be restored.
- Step 3: Muscles, tendons, arteries, nerves and veins are then repaired. Sometimes grafts or artificial spacers of bone, skin, tendons and blood vessels may be needed, too. The grafts can be from your own body or from a tissue bank.
Recovery
Patients have a very important role in the recovery process. Generally, patients should:
- Avoid smoking, as it may cause loss of blood flow to the replanted part.
- Keep the replanted part above heart level to increase circulation.
Other factors that may affect recovery are:
- Age. Younger patients have a better chance of their nerves growing back. They may regain more feeling and movement in the replanted part.
- Area of injury. Generally, more use will return to the replanted part if it is further down the arm.
- Joint vs. non-joint injury. More movement will return for patients who have not injured a joint.
- Severed vs. crushed body part. A cleanly severed part usually regains better function after replantation than one that has been pulled off or crushed.
- Weather. Cold weather may be uncomfortable during recovery, regardless of how well your recovery is going.
Use of the replanted part depends partially on re-growth of two types of nerves: sensory nerves that let you feel and motor nerves that tell your muscles to move. Nerves grow about an inch per month. The number of inches from the injury to the tip of a finger gives the minimum number of months after which the patient may be able to feel something with that fingertip. The replanted part never regains 100% of its original use, and most doctors consider 60% to 80% of its original use an excellent result.
Rehabilitation
For replant patients
Physical therapy and temporary bracing are important to the recovery process. From the beginning, braces are used to protect the newly repaired tendons but allow the patient to move the replanted part. Therapy with limited motion helps keep joints from getting stiff, helps keep muscles mobile, and helps keep scar tissue to a minimum.
Even after you have recovered, you may find that you cannot do everything you wish to do. Tailor-made devices may help many patients perform special activities or hobbies. Talk to your physician or therapist to find out more about such devices. Many replant patients are able to return to the jobs they held before the injury. When this is not possible, patients can seek assistance in selecting a new type of work.
For amputees
If you have completed an amputation, therapy and rehabilitation also play a large part in recovery. For the missing part, a prosthesis may be worn (a device that substitutes for a missing part of the body).
Emotional recovery
Replantation or amputation can affect your emotional life as well as your body. When your bandages are removed and you see the replanted or amputated part for the first time, you may feel shock, grief, anger, disbelief or disappointment because the body part does not look like it did before. These feelings are common. Talking about these feelings with your doctor often helps you come to terms with the outcome. Your doctor may also ask a counselor to assist with this process.
© 2014 American Society for Surgery of the Hand

An active scar may be red, raised, firm, and thick. Scar tissue may involve only the superficial skin, or it may involve the deeper tissues beneath the skin, including nerves and tendons. Scar formation is a normal response following any injury or surgery; it is the way the body heals injured structures. Scars can become overly sensitive and can limit motion and function.
Your hand surgeon or hand therapist may recommend a variety of scar treatment once your injury is healed, incisions are closed, and sutures are removed. Timing of scar treatment varies depending on the type of injury or surgery. Scar management treatments may include:
- Scar massage: Can help reduce sensitivity and loosen any adhesions to deeper structures, especially tendons and joints. Scar massage helps to produce a scar that is smooth and moveable.
- Early controlled exercise programs: Can prevent stiffness of nearby joints and keep tendons gliding under the skin.
- Silicone gel: Can be placed on the scar in sheets or in liquid form for adults (often at night), and taping/wrapping of the scar can help reduce swelling and tension.
- Massage, vibration and rubbing the scars with various textures: Can help overly sensitive scars, which occur when the nerves in the skin and deeper tissues are affected by the injury or surgery. The scar may also be submerged in various slightly abrasive particles. The goal of this treatment is to reduce scar sensitivity and to help the skin and nerves become tolerant of the normal forces of everyday living. This process of “desensitizing” the scar can take up to 4 months and is best initiated as soon as the skin and repaired tissues have adequately healed.
- Injections or surgery: Can be effective for special scar problems, such as burn scars/contractures or keloids that require more vigorous treatment. Special gloves or topical treatment may be recommended for burn scars.
Some scars take up to a year to become completely mature. Therefore, some scar revisions may not be offered until a year after injury/surgery. Scars have completed the healing process when they are light in color, smooth, supple, and no longer sensitive to touch. While scars are young and in the healing phase (pink, red, raised, thick, and sensitive) they should be protected from the sun as sunlight can damage the fragile scar and ultimately darken its color.
Scar Healing
After the skin and deeper tissues have healed, the scar goes through four different stages of healing:
- Hemostasis (bleeding stops)
- Inflammation
- Repair
- Remodeling (or maturation) of the scar tissue
By the time the skin heals within seven (arm/forearm) or 10-12 days (hand/fingers), the first two stages have already taken place. Although the initial skin scar may be minimal, the scar will often enlarge and become more reddened over the following 4-6 weeks. An active scar is typically red, raised, firm and thick. Sometimes this change is misinterpreted by the patient as a possible infection. However, with a normally healing wound, there is no drainage or blistering. The outermost layer often loosens with the deeper layers remaining intact and, while this can give the appearance of “opening up,” it is normal.
Following the swelling/reddening phase, the wound gradually reduces in size and color over the next 2-3 months (Figure 1). Later, the scar becomes soft and has a more natural color in most individuals.
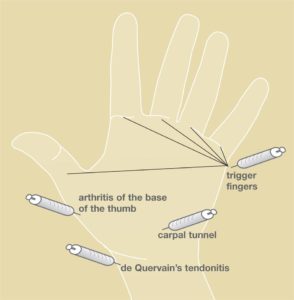
Steroid injections can be used to treat some problems in the arm and hand. These can include trigger fingers, tendonitis, carpal tunnel syndrome, arthritis, tennis elbow and rotator cuff tendonitis. These injections usually contain cortisone and a numbing medicine.
Cortisone is a steroid normally produced by your body, and it is a powerful anti-inflammatory. Corticosteroids tend to shrink, thin and slow things down. These steroids are different from anabolic steroids, which have been abused by athletes to build muscle and enhance performance.
Results
The injection should take effect within a few days, and the benefits can last for many weeks; however, results are not the same for everyone or every problem. For some conditions, one injection solves the problem. For others, several injections may be required. There is no set rule as to how many injections a person can get. Your doctor might limit the number of injections because repeated cortisone can damage tendons and/or cartilage.
Side Effects
The most common side effect of steroid injections is known as a “flare.” This pain is felt for one or two days after the injection. It can be treated with ice and by resting the area injected.
Other side effects might include:
- A rise in blood sugar level for diabetic patients for about five days
- Thinning of the skin
- “Lightening” of the skin at injection site (more common in patients with dark skin)
- Weakening of tendons, making them more likely to rupture
- Allergic reactions (rare)
One of the rare but more serious problems is an infection, especially if the injection was given into a joint. If you notice redness, extreme pain or heat at the injection site, or if you have a fever greater than 101° after an injection, you should call your doctor.
© 2015 American Society for Surgery of the Hand

Many different conditions can be treated by this procedure. It is necessary when a certain muscle function is lost because of a nerve injury. If a nerve is injured and cannot be repaired, then the nerve no longer sends signals to certain muscles. Those muscles are paralyzed and their muscle function is lost. This surgery can be used to attempt to replace that function. Common nerve injuries that are treated with this procedure are spinal cord, radial nerve, ulnar nerve, or median nerve injury.
Such surgery may also be necessary when a muscle has ruptured or been lacerated and cannot be repaired. Common muscle or tendon injuries that are treated with this surgery are tendon ruptures due to rheumatoid arthritis or fractures and tendon lacerations that cannot be repaired after injury.
This surgery may also be needed if a muscle function has been lost due to a disorder of the nervous system. In this situation, the nervous system disease or injury prevents normal nerve signals from being sent to a muscle, and imbalance in hand function occurs. The muscle imbalance or muscle loss due to nervous system disease may be treated with tendon transfers. Common nervous system disorders treated with this surgery are cerebral palsy, stroke, traumatic brain injuries, and spinal muscle atrophy.
Finally, there are some conditions in which babies are born without certain muscle functions. In these situations, the missing muscle functions can sometimes be treated with this procedure. Common conditions treated this way include hypoplastic (underdeveloped) thumbs and birth brachial plexopathy (nerve problem with paralysis).
Procedure
Below the elbow, there are over forty muscles. Each different muscle has a different function. For example, there are 9 muscles that move the thumb. Each muscle has a starting point (origin), and tapers down from its muscle belly into a tendon that then attaches onto bone (insertion) in a specific place; when the muscle fires (contracts), it causes a certain motion (action).During this surgery, the origin of the muscle is left in place; the nerve supply and blood supply to the muscle is left in place. The tendon insertion (attachment) onto bone is detached and re-sewn into a different place. It can be sewn into a different bone, or it can be sewn into a different tendon. After its insertion has been moved, when the muscle fires, it will produce a different action, depending on where it has been inserted.
Alternatives
You can discuss other treatment choices with your hand surgeon. Other options may include repairing the nerve that has been injured, or repairing the tendon or muscle that has been injured. In some cases, tendon grafts can be used, in which a portion of intact tendon is removed, without its muscle, and used to bridge a gap in an injured tendon. In other cases, tendon lengthening or bone fusions may be necessary as part of reconstructing hand function.Risks
All surgery has some risk, although those risks may be small. All surgeries produce a surgical scar. Surgical incisions may develop infection. All surgeries require the use of anesthesia, and will require a complete history and physical examination by your primary care physician to determine if you have medical risks associated with anesthesia. Evaluation by the anesthesiologist will help outline your risks and options.When a tendon is transferred and sewn into another position, the tendon transfer will need a period of time to heal, usually about one to two months. A splint or cast may be used, followed by therapy to teach you the new tendon function. Finally, exercises will be needed to strengthen the muscle after your hand surgeon feels the tendon transfer has sufficiently healed. You will need to follow post-operative instructions. Movement too early can lead to rupture of the tendon transfer. Movement too late can lead to excessive scarring of the tendon with resultant stiffness. Discussion of your individual case with your hand surgeon will help you further understand the risks and benefits associated with this surgery.
Example
After a fracture of the wrist, the fragments of bone associated with the fracture may erode the tendon that straightens the tip of the thumb. In this situation, the thumb tip would not be able to move upward (extend). The muscle that extends the tip of the thumb is the extensor pollicus longus (EPL) (see Figure 1). In this example, the EPL tendon typically cannot be directly repaired because it is too frayed. There are two muscles that extend the index finger. Just like the body has two kidneys, so that one can be spared if necessary, the body also has two tendons that extend the index finger. One tendon is left intact on the index finger so that it won’t lose extension, and the “extra” tendon can be transferred over to the thumb to replace the lost function. The tendon insertion of the “extra” index finger extensor tendon (Extensor indicus proprius—EIP) is detached. The EIP tendon is then re-directed and sewn into the thumb bone or thumb tendon (EPL).After this type of surgery, a splint or cast is used for one month, after which supervised therapy may be started to re-learn how to use the transferred tendon to extend the thumb. Gentle movement with a protective splint may be used for an additional month. If adequate progress is made, the therapy may be advanced one month later to re-learn activities and to strengthen the muscle, with restoration of the ability to extend the thumb. A supervised hand therapy program for retraining the muscles is extremely important to achieve the best possible function.
Figure 1: Example of this surgery.
© 2011 American Society for Surgery of the Hand. Developed by the ASSH Public Education Committee

In the last five years, the wrist (Figure 1) has become the third most common joint to undergo arthroscopy, after the knee and shoulder. Because the cuts used with this procedure are smaller and disrupt less soft tissue than typical surgery, pain, swelling and stiffness are minimal, and recovery is often faster.
Procedure
Your doctor can see the ligaments and cartilage surfaces of bones with wrist arthroscopy. Some parts of ligaments have a good blood supply and can be repaired and heal, whereas other parts do not have a blood supply and don’t heal, so they are removed.
During the procedure, a small camera fixed to the end of a narrow tube is placed through a small cut in the skin directly into the back of the wrist joint (Figure 2). The image is projected onto a television screen for better viewing. Several small cuts are used to allow the surgeon to place the camera in a number of positions to see the cartilage of each bone, the ligaments and the joint lining called synovium.
Risks
Risks of this surgery can include but are not limited to:
- Infection
- Damage to nerves, tendons or cartilage
- Stiffness or loss of joint motion
Stiffness can be addressed post-surgery with rehabilitation.
Recovery
After your surgery, you will be placed in a bandage that may prevent wrist motion. This will protect the area and provide pain relief. Arthroscopy most likely does not require an overnight hospital stay. Fingers should move freely, and finger movement is often encouraged to limit swelling and stiffness. Your surgeon will provide instructions on caring for your wound, therapy, safe activities and any work or exercise restrictions. Elevating the wrist is important to prevent swelling and pain after surgery.
© 2014 American Society for Surgery of the Hand
 — Logo")
 — Logo")
 — Logo")